Over the last few months I’ve learned of more people who have been strictly following a carnivore diet (exclusively muscle meats) for five or more years. Not at all surprisingly, they are doing very well. Combined with all the evidence I’ve included in my eBooks, and with my own 5+ years on a vitamin A free diet, it’s clear that the theory of vitamin A being an essential nutrient is patently wrong. According to the vitamin A theory these people, and myself, should have gone blind years ago, and had their skin and all their internal organs self-destruct and otherwise disintegrate. Not only has that not happened, it’s just the opposite. These people are thriving and healthier than many of their peers.
As I wrote about in my P4P eBook, the foundational studies used to establish the “it’s a vitamin” concept were pretty much just garbage science. I’m sorry, but poisoning a couple dozen rats to death does not prove the existence of a “vitamin”.
Although many people are now conceding this fact that it’s not a “vitamin” needed by adults, there are still people clinging to the claim that it’s essential for embryo development. I find that claim and position so strange because we know that too much vitamin A will cause horrible birth defects and often times spontaneous abortions. Yet, some people continue to believe that nature is so foolish to establish a critical dicey dependency on a highly toxic molecule to facilitate proper embryo development. This is their last bastion of hope in clinging to the claim that vitamin A is still somehow a “vitamin”.
It gets even more perplexing once you know that the so-called “active form” of vitamin A is 13-cis-retinoic acid (isotretinoin aka Accutane) and all-trans-retinoic acid (tretinoin). These thought to be “active forms” of vitamin A are as toxic to the human fetus as is thalidomide. The FDA has established “black box” warnings that a fetus exposed to “ANY” amounts of isotretinoin is at extreme risk for developing birth defects. Astonishingly, in the face of those facts the established “science” claims that a fetus somehow needs this exact same compound to properly develop. How do we square up these diametrically opposing statements? Of course, we can’t and clearly then there’s something seriously wrong with that claim.
Like with the early rat studies from the 1920s that supposedly conclusively established vitamin A to be a vitamin, we need to analyze the modern day studies that were used to prove the need for retinoic acid in fetal development. Here’s an overview of the premier studies that “unequivocally” established the critical dependency on retinoic acid during embryogenesis.
Symposium: Functional Metabolism of Vitamin A in Embryonic Development Vitamin A and Embryonic Development: An Overview Maija H. Zile Department of Food Science and Human Nutrition, Michigan State University, East Lansing, MI 48824-1224 J. Nutr. 128: 455S–458S, 1998
I find it troubling that so much of medical “science” relies almost exclusively on “studies” such as this. The way I see it, these “studies” are a complete cop-out for genuine, critical and logical thinking. Depressingly, it only takes a few minutes of thinking to see the flaws in this one. It’s just more bad “science” layered upon many shaky assumptions. The parallels here with what happened with the Wolbach and Howe study back in 1925 are also rather remarkable.
TISSUE CHANGES FOLLOWING DEPRIVATION OF FAT SOLUBLE A VITAMIN.
BY S. BURT WOLBACH, M.D., AND PERCY R. HOWE, M.D. From the Department of Pathology, Harvard University Medical School, and the Forsyth Dental Infirmary, Boston. Received for publication, September 4, 1925
The Wolbach and Howe study was conducted for about a 10-week duration. At the end of that duration, most of their test animals were either seriously diseased or had died. The fundamental conclusion from that study was that the animals had suffered their devastating tissue and organ disintegration as a consequence of a vitamin A deficiency.
One of the biggest issues with the Wolbach and Howe study is that although they acknowledged that other contemporary researchers were getting the completely opposite results, Wolbach and Howe simply made up excuses to ignore those inconvenient facts. But, the bigger issue is that they delusionally assumed that they were working with complete information. Of course, they were not. They failed to appreciate that washing casein in alcohol and heat treating it at high temperatures could have toxified it. And, yes, somehow casein can become remarkably toxic.
Casein is a Carcinogen – Dr. T. Colin Campbell
Topic #1 – Casein is a Carcinogen. Really?
Many people have heard me say, “Casein [the main protein of cow’s milk] is the most relevant chemical carcinogen ever identified.” Guilty, as charged. Many times I’ve said this. For the sake of this discussion, let’s call it an hypothesis, that is, “Casein causes cancer”.
How can the most revered of all nutrients increase the most feared of all diseases? “Heresy”, the mob might shout.
But it’s true. In my laboratory research conducted over a quarter century, funded by taxpayer dollars with findings published in the very best journals, we studied this effect in many ways at a most fundamental, cellular and sub-cellular level as much research as for any other chemical deemed to be a carcinogen.
Campbell was not alone in this research and in his findings. There were similar studies conducted at the University of Illinois at Chicago that replicated these results. Very interestingly, although Campbell was mostly focused on liver cancer, the Chicago researchers found that casein was a very potent carcinogen in quickly initiating and promoting breast cancer in animals.
After Campbell, and the other researchers at the University of Illinois, had made this discovery about the rather incredible toxicity of casein there should have been some rather intensive follow-up research as to exactly why a milk protein could be so toxic. After all, since most mammals start out in life being breastfed, how could milk be such a potent cancer causing agent? On the surface of it, that doesn’t make any sense. However, when you get deeper inside of it and discover the vitamin A molecule contained within it, it becomes much more plausible. I have no doubt the standard casein based lab chow used in Campbell’s et al rat experiments was heat treated. Heat treating it is simply necessary to sterilize it from potential bacterial contaminants.
Except, with this revelation from Campbell et al about casein being a powerful carcinogen, why hasn’t anyone gone back in time and questioned the validity of the 1925 Wolbach and Howe study? After-all, they too used casein in their experiments. Couldn’t their animals have suffered from ‘the most relevant chemical carcinogen ever identified” rather than have suffered from a vitamin deficiency? Additionally, why has no one ever bothered to try to understand why the symptoms of the so-called vitamin A deficiency condition are a perfect match for those of its toxicity symptoms? Isn’t that odd?
I wrote about Dr. T. Colin Campbell’s China study in my P4P eBook. I really liked the China Study, and I still think that it’s a worthwhile read. Two very important conclusions Campbell makes in his book are:
Food is at the root cause of chronic disease (and particularly so for cancer).
The medical sector and medical science is driven by greed and is rife with corruption.
His third, and most important conclusion, is slightly correct, and mostly wrong. He concluded that it’s the milk protein, and therefore by erroneous extrapolation, that most animal sourced proteins are the culprit. However, it’s not the milk protein at all that’s the real culprit. Rather it’s the highly toxic oxidized retinol molecule that’s cased-in the casein that’s to blame.
Aside: Quite remarkably, this information about the standard lab “rat chow” based diet that included sterilized casein being a potent carcinogen probably invalidates most of other animal based studies that have used this same feed. That’s likely thousands of studies in all aspects of medical research now being highly questionable, at best.
Let’s get back on track here with the more modern day studies that “unequivocally” proved the need for retinoic acid (RA) in embryogenesis.
Vitamin A and Embryonic Development: An Overview Maija H. Zile Department of Food Science and Human Nutrition, Michigan State University, East Lansing, MI 48824-1224 J. Nutr. 128: 455S–458S, 1998
ABSTRACT: Vitamin A is an essential micronutrient throughout the life cycle. Its active form, retinoic acid via retinoid receptors, is involved in signal transduction pathways regulating development. Both the lack and excess of vitamin A during embryonic development result in congenital malformations. Approaches to examine the function of vitamin A in embryonic development have included treatment with excess retinoids and the use of retinoid receptor knock-out mice, which have provided important insights into the complexity of the retinoid signaling system.
The entrenched current theory is that RA is a “metabolite” of vitamin A. What’s documented, and then simply blindly repeated hundreds of times over, is that RA is the downstream molecular product needed to “differentiate” our stem cells. However, even under a tiny amount of scrutiny that “theory” is nothing more than an assumption. One of the red flags that should pretty much jump off the page at us is that many of the horrible skeletal defects attributed to RA deficiencies are a perfect match for RA toxicity (or mere exposure to RA). They state:
The overlap of the teratological symptoms of vitamin A deficiency and excess indicates common targets and a critical role for A in the development of many organs.
Doesn’t that sound familiar? And then they make this statement.
It is important to keep in mind that the developing embryo is very sensitive to a lack as well as an excess of retinoids.
So, here we go again, having just a touch too much RA or too little RA and you get the same teratological results. Odd huh?
Of course designing an experiment to prove the effects of RA deficiency is rather difficult. They can’t just feed experimental animals a diet deficient in all sources of vitamin A because they “know” that the animals will quickly die, let alone allow them to breed through one or more reproductive cycles. So, what the researchers in this study have done is used genetically modified “knock-out” mice. The gene knock-out changes their DNA so that they will be unable to produce the retinoic acid receptors (RARs) needed to utilize RA.
Retinoic acid is now generally recognized as an important signaling molecule that as a ligand to its nuclear receptors, the RARs alters gene expression at the level of transcription (Gudas et al. 1994, Mangelsdorf et al. 1995, Pfahl and Chytil 1996, Roberts and Sporn 1984).
So, basically, their thinking is to disrupt the RA metabolism pathway so as to block the final critical step of having RA invoking those 500+ random gene expressions.
A recent approach to answering questions about the functions of vitamin A in development has been the use of transgenic mice with changes in retinoid receptor gene structure (Boylan et al. 1995, Chambon 1993, Giguere et al. 1996)
Normal vitamin A metabolism pathway
The normal “receptor” pathway
Knocking out the RARs and RXRs Using their gene “knock-out” mice they’ve taken out the RARs, and RXRs.
The “knock-out” applied
The “disrupted” vitamin A metabolism pathway
Do you see the “disrupted” pathway? Actually, neither do I.
But, sure enough, with that induced mutation they find exactly what they are looking for. Disrupting the RA metabolism pathway results in the development of horrible and catastrophic skeletal and organ defects. Of course, as predicted, their conclusion is that RA is essential for embryogenesis.
Many of the abnormalities in these mutant mice resemble those observed in the fetuses from the vitamin A deficient animals reported earlier.
Obviously, there are some huge flaws with these experiments and in their logic. Firstly, what if that cellular process of dealing with RA is not one of “metabolism” but rather one of catabolism and detoxification? Of course, when a cancer patient is given the RA “treatment” their body is not metabolizing it, it is frantically detoxifying it. In the process, the result is the horrific widespread destruction the “medication” causes in almost all patients.
Differentiation syndrome (DS) is most current term; Occurs in Acute promyelocytic leukemia patients undergoing ATRA treatment (Tretinoin, Vesanoid).”
Differentiation Syndrome is a life-threatening complication of induction chemotherapy for patients with acute promyelocytic leukemia (APL). Manifestations of this syndrome include fever, hypoxemia, edema, and, in the past, has been referred to as “cytokine storm”.
Yet, somehow we are supposed to believe that the exact same chemotherapy drug is needed for proper embryogenesis. That should sound rather ludicrous to everyone.
Next, we need to consider what if the gene “expressions” are really manifestations of gene damage? But, most glaringly, what they haven’t proven at all is the condition of RA deficiency. No, there is still vitamin A and RA in the cell. They’ve only blocked its assumed to be one-and-only pathway. However, in no way have they limited the availability of RA to bind with and cause DNA damage. Obviously, even without the RARs, that RA molecule is still free to float around the cytoplasm and bind to the DNA/RNA. Therefore, what they’ve really done in this study is just proven that RA is very toxic to the embryo even when the retinoic acid receptors are not available. That outcome is not at all surprising because we now know that RA fractures and fragments DNA.
DNA fragmentation induced by all-trans retinoic acid and its steroidal analogue EA-4 in C2C12 mouse and HL-60 human leukemic cells in vitro Raghda S. Alakhrasa, Georgia Stephanoua, Nikos A. Demopoulosa*, Konstantinos Grintzalisa, Christos D. Georgioua and Sotirios S. Nikolaropoulosb
Abstract: We have recently shown that retinoic acid induces micronucleation mainly via chromosome breakage.
Next, what about the long-held assumption that the one-and-only pathway of RA metabolism is via the RARs? Well, it turns out to have been the wrong assumption.
Retinoic acid induces apoptosis by a non-classical mechanism of ERK1/2 activation Alfeu Zanotto-Filho, Martin Cammarota, Daniel P. Gelain, Ramatis B. Oliveira, Andres Delgado-Cañedo, Rodrigo J.S. Dalmolin, Matheus A.B. Pasquali, José Cláudio F. Moreira
Abstract: Even though RA is involved in differentiation and apoptosis of normal and cancer cells, being sometimes used as adjuvant in chemotherapy, its mechanisms of action involve multiple overlapping pathways that still remain unclear. Recent studies point out that RA exerts rapid and non-genomic effects, which are independent of RAR/RXR-mediated gene transcription.
And they go on to state:
Classically, it has been described that the effects of RA are mediated by ligand-dependent activation of RA receptors (RAR) which act directly as transcription factors modulating gene expression by interacting with RA response elements (RARE) in DNA (Kastner et al., 1995). A number of RA target genes have been identified and many of them are associated with apoptosis and differentiation (Kastner et al., 1995; Pfahl, 2003). On the other hand, recent studies point out that RA modulates signaling pathways in a manner independent on retinoid nuclear receptor-mediated gene transactivation; this has been described as ‘‘non-classical” or ‘‘non-genomic” action of RA.
With that bit of new information, there’s now no legitimate evidence that RA is needed for embryogenesis. And of course there isn’t. How could anyone be so credulous to believe that a molecule as toxic as thalidomide to the developing fetus, and one that’s proven to fracture DNA, cause cancer, cause 500+ other variations of DNA damage, and to induce rapid apoptosis is somehow needed for embryo development?
Child exposed to Thalidomide
Moreover, it’s rather clear that the RARs are one of the last defense mechanisms against RA’s toxicity.
Then, we need to ask the next obvious question. If the RARs are really part of the detoxification pathway, then what’s the result of that pathway being disrupted? It’s cancer!
The disruption of RA signaling pathways is thought to underlie the etiology of a number of hematological and non-hematological malignancies, including leukemias, skin cancer, head/neck cancer, lung cancer, breast cancer, ovarian cancer, prostate cancer, renal cell carcinoma, pancreatic cancer, liver cancer, glioblastoma and neuroblastoma.
Retinoic acid receptors: From molecular mechanisms to cancer therapy
Alessandra di Masi, Loris Leboffe a, Elisabetta De Marinis b, Francesca Pagano, Laura Cicconi, Cécile Rochette-Egly, Francesco Lo-Coco , Paolo Ascenzi, Clara Nervib, 2014 http://dx.doi.org/10.1016/j.mam.2014.12.003
This finding is similar to the report I referenced in my Breast Cancer eBook where the researchers found that cancer tissues are depleted of the needed alcohol dehydrogenase enzyme. So, basically, it looks like when a cell can no longer defend itself from RA, it can become cancerous. Once again, that should not be a surprise to anyone because of the hallmarks of cancer are damaged DNA and rapid cell mitosis, and that’s exactly what RA does to cells. Hmm? What are the chances that the RARs and RXRs are in actuality the precursors proteins to the RBPs that we now know cells form around retinol and RA and then eject out of itself?
Anyhow, it’s quite remarkable how the thinking process and conclusions in the Vitamin A and Embryonic Development study “unequivocally” proving that RA is needed for embryogenesis parallels that of the 1925 Wolbach and Howe study. Both teams find exactly what they are looking for and they both ignore huge amounts of evidence by other research and knowledge contradicting their conclusions. Most disturbingly, they just don’t seem to apply common sense to alert them to the fact there’s something drastically wrong with their conclusions. And, like with Wolbach and Howe back in 1925 these researchers are so sure of themselves that they completely ignore the contradictory findings from their contemporaries. I say that because ten years prior to them conducting these elaborate genetic knock-out studies, the HHS was quickly (in just 10-14 days) poisoning young mice to death with the very same molecule they are claiming to be essential for embryogenesis.
United States Patent 4,649,040
The United States of America as represented by the Department of Health and Human Services, Washington, D.C. Mar. 10, 1987
Therefore, it’s all quite ridiculous and almost absurd. I mean seriously, with that information how could anyone continue to believe that a proven lethal and teratogenic poison is needed for embryogenesis?
Quite interestingly, both the studies by T. Colin Campbell in the 1990s, and that of Alessandra di Masi’s in 2014 both point to cancer causation, and even specifically to breast cancer causation. Amazingly, Campbell was able turn on and off cancer progression just by turning up or down on the amount of casein being included in the animal diet. That’s a pretty good indication that cancer is being fueled by the ongoing supply of vitamin A.
Yet, as I wrote about in P4P, very disturbingly, when other researchers do find direct links with vitamin A and the retinoids causing cancer, they conceal it and cover it up. That isn’t science. I view it as criminal negligence, at best. It sure begs the question: how could so much of medical science be so screwed up? Is this deliberate scientific propaganda and manipulation to corral us into disease? Of course, there’s huge amounts of money being made everyday in cutting off the breasts of women. But, no one’s going to make a dime off of breast cancer if we reveal the true root cause of the disease, and can therefore prevent it. T. Colin Campbell was correct; corruption is not only endemic to modern medical science, it appears to be institutionalized in the medical establishment.
I wouldn’t be so snarky about it if this was some harmless mistake. But, it’s not. And, we are not just talking about melanomas and breast cancers either. The USA now has the highest rates of birth defects and spontaneous abortions in the world. We’re talking about nearly a million people in just the USA now living with birth defects. With the current CDC estimates that birth defects are occurring at a rate of 1 in every 33 infants born in the United States this represents an ongoing national disaster. Coincidentally, that 1/33 rate is about on par with the current rates of autism too.
The human body is many thousands of times more advanced than the current state of medical science. This is clearly evidenced by the fact that the more health interventions and drugs pushed onto our populations the sicker we’ve become. And we’ve become vastly sicker, and on a massive scale too. That alone is conclusive proof that many of the so-called experts have no freaking clue what they are doing. The human body was and is perfect. We just need to learn how to stop chronically poisoning it. In order to do that we need to know when a bogus “vitamin” is in fact simply a poison.
I’ve now crossed the nine-year point on my vitamin A elimination diet experiment. I’m sorry to disappoint some folks, but I’ve not died, I have not gone blind, and I’ve absolutely no signs or symptoms of vA deficiency.
Other than that, like with last year’s update, I don’t have much new to report on health wise. This past year for me has been pretty much a steady state of good health. The only noticeable change has been that I feel my energy level is a bit higher and more consistent throughout the day than compared to last year.
Diet
I’m continuing with my standard prison food diet. The only change I’ve made is that I often swap out the rice for a white sourdough bread. This change was mostly due to the concern of getting too much arsenic from the rice. However, with the bread there’s a similar concern with glyphosate. Therefore, I now bake my own bread using a locally grown organic flour that’s glyphosate free. However, I do have a preference for rice and still eat it at least a couple of times per week. I just usually cook it using the parboiling technique.
Some specific health indicators:
Vision
My vision remains excellent. I feel that my vision has slightly improved from last year, but I haven’t had an eye exam to measure it. My night vision is very good too. I’ve had no episodes of reduced night vision.
Body Weight and Strength
My weight remains very steady. My strength in the gym remains excellent. I’m cycling more now that it is summer. I try to get in about 20 km per day.
Skin
Overall, I’d say my skin condition / health is about the same as it was last year. However, the age spots on my face have significantly faded this year. Over the years these age spots have cycled through periods of different variations of darkness. After about the first three years of my elimination diet the age spots had faded maybe by about 50%, but with no significant change in their size. Then, at about year five they once again became quite a bit darker again. Those changes in darkness might just have been due to my face being exposed to varying amounts of sunlight over the seasons. But, this year the age spot on the right side of my face has shrunken down to almost nothing. Originally, it was about the size of a dime. Now, it’s about 1/10th that size. I expect that it will be completely gone in a few more months.
Unfortunately, I don’t have a good before picture of that age spot, but you can somewhat see it in this video interview with Judy Cho.
The age spot on the left side of my face has also reduced in size. It’s now about one half its original size. But, the damage to the skin there is much deeper and more severe, so I expect that it might not ever fully disappear.
Other:
I continue making plasma donations, and I’m now on donation # 38.
My dental health continues to be very good, with more progress on reversing gum recession. Of course, that improvement has been totally unexpected and most dentists probably consider it to be just impossible.
Another surprising change over the years has been the way my body regulates temperature. I’m now pretty much never too cold or too hot. I’m very comfortable in hot weather and sweat very little, and like not at all until I’m in very hot and direct sunlight for like 20 minutes or more. Even if I cycle 20 km in bright sunny weather I don’t sweat. And somewhat likewise for winter weather. When I go skiing in the cold temperatures (say -20°C ) I’m perfectly comfortable. And since I basically don’t sweat much at all, my feet remain completely dry in my ski boots all day long. That’s a huge factor in dealing with cold winter weather.
The realistic timeframe for health recovery
One of the most surprising things to me is that even after these 8-9 years I’m still seeing these small improvements. Clearly, making a full recovery from vA toxicity can take a very, very long time. I had no idea about that when I first started. Of course, I also had no expectation, or even hope, that a vA elimination diet would yield any results. So, I’m very grateful for the results I’ve had, regardless of how long they’ve taken.
Although using an elimination diet alone does work, obviously we sure haven’t figured out the best and safest way of recovering from vA toxicity and its damage. Realistically, we are still in the early days of figuring it out.
This has got me thinking more about the real timeframe and why it takes so long. I guess it kind of makes sense if we look at it from the following perspective. We are not just talking about reducing or eliminating excess vA from our liver and tissues. No, that’s only half the battle. The second half is then allowing the body enough time to repair all the damage that has resulted from the prolonged vA toxicity. Therefore, if we consider:
It usually takes decades of vA accumulation to result in disease. In my case I now know I started to have symptoms of vA toxicity in my mid 20s. Yet, it wasn’t until age 46 that I really got into trouble with CKD. And then it wasn’t until age 54 that the eczema showed up. Therefore, we shouldn’t be surprised to see that it can take about half those 30 years of over accumulation of vA to de-accumulate it and to heal the body.
We know that it takes about 18 years to fully grow an adult human body. And that’s during the optimal growth years of our lives. Now as adults, say in our 40s, 50s and 60s, after having a chronic disease condition for an extended period of time the body has been significantly damaged. To what extent the body’s tissues are degraded, malformed, damaged, atrophied etc is going to be highly variable and individual. But, in my case I’d guess it to have been about 50% damaged. Therefore, at my age I don’t think I should be too surprised to see that it can take a decade or more to repair and rebuild that amount of damaged tissue. Of course, it also might not be even possible to ever fully recover.
Additionally, different aspects of my health have improved at different rates. I’ve made the following sketches approximating that progress. The health scale is from 0 = death to 100 = perfect health for my age. Generally, my overall health recovery has been a slow, but mostly progressive, process with a few periods of relapses / reversals.
Whereas, my joint health made a much more dramatic improvement. My joint health hugely improved almost literally overnight (on day 21 of my diet) and has never regressed.
The recovery of my skin health has proven to be the slowest and most problematic. I’ve had many setbacks and relapses, and of course with different areas of my skin responding / recovering at different rates. Since the skin on my hands was the area worse affected by eczema, and also severely damaged by steroid creams, it has been the slowest to fully recover.
Anyways, as I mentioned in my Tackling the Detox Setback blog post, I think I might have recovered faster if I had continued taking soluble fibre and activated charcoal. And maybe I could have been more consistent with zinc supplements. But, even that is risky by itself. So, combined with being generally paranoid of supplements I didn’t want to risk messing up my gains.
Repeating the 1925 Wolback and Howe study
For the last three or four years I’ve talked about wanting to repeat the 1925 Wolback and Howe study. That is because that’s one of the standard things you do in science; repeating experiments done by others and proving that we can replicate their results or not. Therefore, I was originally planning on having a university repeat the study using small animals. When the pandemic hit those plans were put on hold.
Then, I was thinking that we probably don’t need to do the small animal experiment at all. If we conducted some lab testing of casein samples heated in alcohol and verified that retinoic acid is indeed produced in the process then that would be sufficient. Finding retinoic acid in casein itself would completely disprove Wolback and Howe’s fundamental claim that their rat feed was vA free.
Of course, I went looking to see if I could find existing research on the heating of casein. At first I could only find reports about the pasteurization of milk mysteriously reducing its vA content by about 30%. The reason I say mysteriously, was because they weren’t asking or explaining what happened to that missing 30%. That unasked question being: what did the missing vA convert into?
The binding sites of retinol and retinoic acid with milk α-and β-caseins were determined, using constant protein concentration and various retinoid contents. FTIR, UV–visible and fluorescence spectroscopic methods as well as molecular modelling were used to analyse retinol and retinoic acid binding sites, the binding constant and the effect of retinoid complexation on the stability and conformation of caseins. Structural analysis showed that retinoids bind caseins via both hydrophilic and hydrophobic contacts with overall binding …
The number of bound retinol molecules per protein (n) was 1.5 (±0.1) for α-casein and 1.0 (±0.1) for β-casein, while 1 molecule of retinoic acid was bound in the α- and β-casein complexes. Molecular modelling showed different binding sites for retinol and retinoic acid on α– and β-caseins with more stable complexes formed with α-casein. Retinoid–casein complexation induced minor alterations of protein conformation. Caseins might act as carriers for transportation of retinoids to target molecules.
Caseins play an important role in stabilising retinol, which does not degrade over time or during heat treatments.
So, there you have it. Casein is not only a natural binder and carrier of both retinol and retinoic acid, it actually does so on more than a 1:1 ratio molecule for molecule. Therefore, the 1925 Wolback and Howe study diet was not only definitely not a vitamin A free diet, it was actually quite high in both retinol and retinoic acid.
Wolback and Howe had assumed that they had removed all possible sources of vA in their rat diet because they had removed all the fats. With the “vitamin” thought to be exclusively fat-soluble they wouldn’t have known, or even considered, that the casein protein portion of their lab diet included substantial amounts of it too.
Anyways, that’s it, it’s game over for the 1925 Wolback and Howe study. As suspected, it’s completely garbage science. It’s toast, dead and finished. The same goes for every follow-on study claiming the ridiculous, and fabricated out of thin air, BS that we somehow need this horrible chemotherapy drug to “regulate” our gene expressions. Or that we need it to control our stem cell differentiation, keep us from going blind, dying, and on and on. Those studies, and it’s probably thousands of them, are now all garbage, complete junk “science”.
Not to be too dramatic about it, but these stupid and corrupt “studies” have resulted in the poisoning of hundreds of millions of people, and of course children, from around the world. Unfortunately, and very tragically it continues to go on to this day. I highly doubt the poisonings will ever stop. There’s just too much money being made off of it.
Naturally, many people will be asking how could so many in medical “science” have been so wrong for so long? Well, it’s primarily due to the nature of this field being almost entirely focused on business and profits. There is actually very little genuine interest in real science as far as I can tell. Secondly, we’ll never get more than a few people from the medical “science” field to come to terms with and accept the new fact that vA is not a vitamin, and that it is therefore nothing but a toxin.
No, there’s no way the medical establishment and governments will ever allow that to happen. They’d have to admit that they’ve been (inadvertently or secretly) poisoning most of the human population for the last 50 years. Then, there’s the fact that vA is highly likely the primary driver behind the chronic disease and cancer epidemics. Those are Big Pharma’s annual multi-trillion dollar sacred cash cows. Actually finding the root cause of disease is the very last thing the medical establishment wants to do. “CURE” is a vile and foul four-letter word to the pharmaceutical industry. No, all they want to do is to perpetually “treat” di$ea$e.
No doubt many people will react to those statements equating them to some grand conspiracy theory. Well, many corporations and governments are conspiring almost every single day. That’s their normal operating procedure. It’s just a standard business practice, and technically speaking it’s usually not illegal. Then, if and when something does go wrong they just lie and cover it up. That is absolutely another long established standard operating procedure of governments all around the world. It is not a conspiracy theory, it is a conspiracy fact, because it happens all the time.
In the last few years we’ve all had front row seats witnessing just how the corporate-government conspiracy SOP playbook is applied. And seeing how obscenely corrupt and degenerate it really is. Since the roll-out of the poison needle there’s been a huge increase in excess deaths. In Canada it’s running at about 50,000 excess deaths per year. In the UK it’s about 80,000 excess deaths per year. In the USA it is about 500,000 excess deaths per year. In the EU it’s running at about the same rate. So, we are easily talking about one million or more people who have suddenly and mysteriously died that shouldn’t have. To be clear, this is not conjecture, those numbers are based on government collected and sourced data. Here is a good overview / summary of the situation with the excess deaths.
Of course, the increase in excess deaths is happening in all age groups, including children and youth/ young adults. We had the owner of a casket manufacturing company in the Toronto area do interviews on alternative media about the surge in orders he’s had for child caskets. He said it’s like nothing he’s ever seen before in his 20+ years of being in the business. He said he was even getting bulk orders for the child caskets.
I personally knew one of these innocent young victims. He was my neighbour’s son. We knew him for most of his young 17 years. He was very athletic and played hockey every season with my son. He was a strong, perfectly healthy, happy kid. He had his whole life ahead of him. But, his bright future was abruptly cancelled by the “science”. Similar sequences of events have happened to thousands of young people right across the country, and around the world.
So, what’s been the response from the Canadian government, and actually from all governments all around the world? Silence, absolutely nothing!
What’s been the response from the medical “sciences” community? Silence, absolutely nothing!
What’s been the response from nearly all doctors and pathologists? Silence, absolutely nothing!
What has been the response from mainstream media? Total silence…shh.. crickets…..
How can that be? How can there be ZERO interest from governments to even start to investigate this huge surge in excess deaths, and the deaths of tens of thousands of children? Well, their silence tells us everything we need to know.
Yes, we know exactly why there’s no interest. It’s because they already know precisely what’s going on. Of course there will be no investigations; not now, and not ever. It all needs to be hushed up, covered up and concealed using every and all means possible. Virtually none of our so-called political “leaders” (what a joke) and others in “authority” are going to even mention it, let alone ever admit that they’ve colossally f’d up. Many of these people listed above are also very handsomely paid off (rewarded) for their silence. That is the corrupt standard operating procedure in action.
Of course, we know absolutely what’s happened. It’s the poison needle! I mean seriously, even a child could piece it together. Yet, in the middle of this very serious and real crisis our governments, and law enforcement agencies, are going to do absolutely nothing about it. I’m aware of a police officer in Ontario who wanted to start an investigation, and he was promptly fired. In a somewhat similar case Constable Helen Grus of the Ottawa police force was brought up before a disciplinary tribunal for just accessing a database while starting to look into the pattern of unusual sudden infant deaths (SIDS) in the region in 2021. Can you imagine that a police officer just starting to look into the suspicious deaths of infants is now effectively a crime.
It’s a very dark and dangerous time in our so-called democracies. Clearly, it’s no longer: government for the people, by the people. No, it’s now: government for Big Pharma, by Big Pharma.
What’s next for me?
I’ll continue with my vitamin A elimination diet for the rest of my life. Like, why not?
Although I’ve been a lot less focused on the vitamin A topic over the last few years, I’ve definitely not lost interest in it. I just feel that the vA toxicity issue now has enough momentum behind it that it’s going to take on a life of its own. What’s needed next are more success stories and better guidance on how to achieve safer, more predictable results. I’ve become very interested in another major issue that I feel is just as important, and potentially even more so, than the vitamin A topic. Over the next few years that will be the primary focus of my attention.
Thank you so much for your continued interest and participation in this investigation.
More than 100 million U.S. adults are now living with diabetes or prediabetes, according to a new report released today by the Centers for Disease Control and Prevention (CDC). The report finds that as of 2015, 30.3 million Americans – 9.4 percent of the U.S. population –have diabetes. Another 84.1 million have prediabetes, a condition that if not treated often leads to type 2 diabetes within five years.
Don’t you think there’s a major problem going on here?
That 100 million number should also look familiar. It’s the same as the number of Americans with fatty liver disease slowly creeping up on them. Clearly, something has gone drastically wrong with human health in North America, and worldwide. And, it’s forecasted to just get worse.
The prevalence of diabetes (type 2 diabetes and type 1 diabetes) will increase by 54% to more than 54.9 million Americans between 2015 and 2030; annual deaths attributed to diabetes will climb by 38% to 385,800; and total annual medical and societal costs related to diabetes will increase 53% to more than $622 billion by 2030
To help put that $622 billion dollar cost into perspective, that is almost twice as much as the total amount that all of America spends on gasoline annually. Yes, just the one disease of diabetes is hugely more costly, and of course profitable, than oil! But, that’s still only a fraction of the nearly four Trillion dollars Americans now spent annually on all health care costs. Of course, the human costs and long term suffering are much more devastating. The annual death rate due to diabetes is 2-3 times that of the current Covid-19 disaster. Naturally, we are not talking about just about North America. The diabetes pandemic now afflicts about 500 million worldwide.
If we don’t get this diabetes disease crisis under control it will surely destroy our economy. I do think we can bring this under control… but it’s not going to be easy. Continuing with the current band-aid type treatments is obviously not working. So, to have any chance at effectively turning this crisis around we need to first get to the correct root cause of it.
The last big breakthrough in diabetes research was back in 1921. Canadians Frederick Banting, Charles Best, and James Collip identified and isolated insulin and quickly went on to develop a process for extracting it from animal sourced pancreases. They licensed the patent for that process to the University of Toronto for the princely sum of $1. With that, insulin went into mass production, was priced at pennies per dose, and saved millions of lives. Today insulin is still the primary treatment for the disease. However, insulin is obviously just that; a treatment, and not a cure. And, today the giant pharmaceutical companies have worked their way around that pesky make it free-to-everyone patent and now sell synthetic insulin at what many consider to be extortionary prices.
The question that Banting and Best did not answer was why was the human pancreas failing in the first place? Maybe, like with most doctors today, they too were taught to believe that diabetes and all chronic diseases are just “bad luck”. Sadly, that ridiculous “bad luck” theory of disease causation is very widely accepted and has gone almost unchallenged even today. But, obviously “bad luck” does not cause organs to fail. It’s equally obvious is that the stupid “bad luck” theory is dead wrong because North Americans could not have gotten vastly more “unlucky” over the last several decades. There’s also no way that people living in the American Southeast are significantly more unlucky than those living in the Northwest.
Back in 1921 we did not have an epidemic of obesity and therefore obesity couldn’t be blamed for the cause of diabetes either. And, obesity most certainly can’t be blamed for Type I diabetes since the wasting the disease causes in children is the direct opposite of that. The presumption is that Type I diabetes is just another auto-immune disease, and auto-immune diseases are just more “bad luck”. We are supposed to believe that it’s the confused and rogue immune cells attacking their own host body. Well, if you’ve read my eBooks you’ll know what I think of the “auto-immune” disease theory. In a nutshell, it’s a bunch of rubbish. No, it’s not a confused or defective immune system. Rather, it’s that tissue cells have been poisoned. With their DNA/RNA being poisoned and damaged they then produce defectively structured proteins. To the immune system those defectively structured proteins appear to have come from a foreign source. The immune system then correctly attacks those cells.
To help better understand the root causes of diabetes we need to know that there’s a similar U-shape curve in the incidence rates that so many of the other chronic diseases follow. There’s a high incidence rate in young children, with a drop-off in rate during youth and teenage years, and then a slow progressive climb in rates with age in adults. Therefore, in adults it’s pretty clear that the disease is one of a slow accumulation.
Source: Rogers, M.A.M., Kim, C., Banerjee, T. et al. Fluctuations in the incidence of type 1 diabetes in the United States from 2001 to 2015: a longitudinal study. BMC Med 15, 199 (2017). https://doi.org/10.1186/s12916-017-0958-6
Now visually sync that chart up with the one I presented in my COVID-19 Vulnerability blog post showing the liver vitamin A concentrations by age. Note the huge spike in early childhood.
Obviously, there’s a lag time between the elevated liver vitamin A storage levels and the onset of the disease. Not at all unexpectedly, it does take some time to burn out the pancreas.
More importantly, we need to understand the exponential growth rates in the incidence rates of both Type I and Type II diabetes over just the last few decades. There is simply no way that this can be naturally happening in the human population. Something is clearly causing it to happen. We also can’t confuse something being really common for it being normal. Sure, diabetes is now very common, but in the historical context that is exceedingly abnormal.
Here’s a chart showing the diabetes prevalence rate here in Alberta.
And for across Canada the regional clustering looks like this:
Any disease that exhibits an exponential growth rate and a geographic clustering pattern like this is clearly a poisoning. It’s a slow poisoning from something that is obviously slowly accumulating and or picking away at cells in the body. It’s just that simple.
With the data presented above, if anyone tries to tell you that the root cause of diabetes is somehow rooted in genetics then simply ask them if they finished their grade 9 math.
Okay, now that we’ve agreed that diabetes is the result of a slow poisoning, let’s find out how likely it is that so-called vitamin A is responsible for it.
Type I Diabetes
As shown in the chart above, type I diabetes is most commonly occurring in children. It is considered to be an auto-immune disease where the defective immune system has wrongly killed off the pancreatic beta cells. With that, the pancreas is no longer able to produce adequate amounts of insulin. What “vitamin” do you know of that causes the rapid mitosis and apoptosis of stem cells?
Retinoic acid induces apoptosis by a non-classical mechanism of ERK1/2 activation Alfeu Zanotto-Filho, Martin Cammarota, Daniel P. Gelain, Ramatis B. Oliveira, Andres Delgado-Cañedo, Rodrigo J.S. Dalmolin, Matheus A.B. Pasquali, José Cláudio F. Moreira
Abstract:
Even though RA is involved in differentiation and apoptosis of normal and cancer cells, being sometimes used as adjuvant in chemotherapy, its mechanisms of action involve multiple overlapping pathways that still remain unclear. Recent studies point out that RA exerts rapid and non-genomic effects, which are independent of RAR/RXR-mediated gene transcription.
Yes, that’s the very functional definition of what the active form of “vitamin A” does to our stem cells. So much so, that it is regarded as the essential molecule that’s somehow needed to “differentiate” our stem cells. What does “differentiate” really mean? It means it causes stem cells that normally reside along a basement membrane to quickly mature into adult cells and separate off. This effect and process of vitamin A’s action is abundantly documented in many fields of medical science, and especially so with its use in dermatology and chemotherapy.
Type II Diabetes
Type II diabetes is characterized by the pancreas still able to produce insulin but for some unknown reason that insulin becomes less and less effective. The pancreas tries to compensate for this ineffectiveness by producing even more insulin. The condition is known as insulin resistance.
As with so many other metabolic diseases there’s a circular blame game going on. Many “experts” believe that obesity is the root cause of type II diabetes. But, of course, that can’t be correct because there are many type II diabetics who are lean. Other experts will claim that it’s the diabetes that’s causing the obesity. I think these guys are significantly more correct. But, not precisely correct. I think obesity is the body’s defensive response to a much more sinister and ongoing threatening condition that we need to be protected from. In other words, what if there’s some other driver that’s causing both obesity and diabetes at the same time? Likewise for the assumed to be diabetes caused comorbidities of kidney disease, cardiovascular disease, macular degeneration, dementia / Alzheimer’s, and, and you name it. Is there something else that could cause all of them to happen? Well, you bet there is. Vitamin A toxicity can, and is proven to, cause all these same comorbidities.
Except, what about this insulin resistance condition? What could be causing that? As I wrote about in a previous blog post, researchers are now identifying the association of elevated RBPs with insulin resistance.
“Until 2005, the sole known function for RBP4 was to mobilize retinol from tissue stores and deliver it to vitamin A-responsive cells where it can be converted to retinoic acid for use in regulating vitamin A dependent transcription and functions. In 2005, Kahn and colleagues reported that circulating RBP4 levels affect glucose clearance, with high RBP4 levels inducing insulin resistance (Yang et al., 2005; Graham et al., 2006). Specifically, Kahn and colleagues proposed that adipocyte-derived RBP4 is a signal that contributes to the pathogenesis of type 2 diabetes, linking obesity with type 2 diabetes, as well as other obesity-related metabolic diseases.”
So, retinol is definitely involved in insulin resistance. Next, we need to appreciate that all cellular receptors are actually proteins intrinsically made by the cell. We need to remember that vitamin A (the retinoic acid metabolite) has been shown to cause more than 500 different gene expressions. What are gene expressions? They are changes in the DNA structure that are detectable by variations in the different proteins that a cell manufactures. So, it’s very possible that the failing insulin receptor is just another protein that has been defectively produced as the result of retinoic acid induced gene expressions (a.k.a. DNA/RNA damage).
That outcome is not at all surprising because we now know that RA fractures and fragments DNA.
DNA fragmentation induced by all-trans retinoic acid and its steroidal analogue EA-4 in C2C12 mouse and HL-60 human leukemic cells in vitro Raghda S. Alakhrasa, Georgia Stephanoua, Nikos A. Demopoulosa*, Konstantinos Grintzalisa, Christos D. Georgioua and Sotirios S. Nikolaropoulosb
Abstract: We have recently shown that retinoic acid induces micronucleation mainly via chromosome breakage.
Do you think that that fracturing of your DNA might cause defectively produced insulin receptors and other proteins? I sure do.
How about conducting a Stress Test
As I mentioned in my eBooks, it is very common in engineering to stress test systems and components to their breaking point. Civil engineers do this everyday with concrete samples as a standard quality assurance practice. Jet engine manufacturers will spin new test engines to incredible speeds, and to the point that the engine explodes or otherwise self-destructs. These types of stress tests are very important as they not only tell us at what point a component will fail, it also helps set the safe operating ranges in real-world usage.
Somewhat likewise, if the theory that vitamin A toxicity is responsible for causing diabetes, then we should be able to conduct similar biological stress tests and see if diabetes can be directly induced by it. Thankfully, that stress test has already inadvertently been conducted for us.
The extreme stress test – Accutane
There have been many accounts of people who have developed type II diabetes shortly after taking accutane. It’s even documented as a known “side-effect”.
The effect of isotretinoin on insulin resistance and adipocytokine levels in acne vulgaris patients.
Soyuduru G, Ösoy Adışen E, Kadıoğlu Özer İ, Aksakal AB. Turk J Med Sci. 2019;49(1):238-244. Published 2019 Feb 11. doi:10.3906/sag-1806-44
Conclusions: All data suggests that five months of isotretinoin therapy in AV patients causes insulin resistance and the increase in insulin resistance is not dependent on age, BMI, BFM, and lipid levels of these patients.
Although this diabetes causing “side-effect” of accutane has been reported on for decades now, as usual it is downplayed and mostly ignored by the medical establishment. Here’s a great example:
Association Between Oral Isotretinoin Therapy and Unmasked Latent Immuno-Mediated Diabetes Ilaria Dicembrini, MD, Gianluca Bardini, MD, PHD and Carlo M. Rotella, MD
It is reasonable that latent autoimmune diabetes in adults (LADA) could be clinically revealed by drug-induced insulin resistance. In this case, the only remarkable change of lipid profile consisted in a reduction of HDL cholesterol during isotretinoin treatment; therefore, the previously reported physiopathological hypothesis (1–4) is not completely supported. However, this is the first report of an association between isotretinoin and an unmasking case of autoimmune diabetes.
Isn’t that a brilliant conclusion? Their ridiculous BS excuse is that the diabetes was already patiently sitting there just waiting to be “unmasked” by accutane use. They want you to believe that: No, no, wonderful accutane didn’t cause the disease, it just “unmasked” it. Who could buy such ridiculous nonsense and pharma propaganda? These are MD’s and PhD’s, no less, making such an idiotic claim. What about the many other disease conditions accutane has proven to cause? Were they then just “unmasked” too?
But, my point here is that we now know that many of us are getting small daily doses of “accutane” via our food sourced vitamin A intake. Thus, if a spiked dose of accutane is proven to cause diabetes, then obviously many low doses, but over a longer period of time, can have the same cumulative result. So, it’s just a matter of dose and time.
A lower range stress tests – Gestational diabetes.
“In the United States, about 1% to 2% of pregnant women have type 1 or type 2 diabetes and about 6% to 9% of pregnant women develop gestational diabetes.”
But, why and how does getting pregnant cause a woman to develop diabetes? That seems like a pretty high price to pay for having children. Something that women have been doing for millions of years now. Once again, there’s no way that nature could be that foolish for this to be normal.
Of course, the big assumption made by endocrinologistsis that gestational diabetes is caused by some vague hormonal imbalance. But, they in no way can explain why it only happens to some women. More importantly, it in no way explains why it’s become much more prevalent over the last few decades and the large regionally disparities in incidence rates.
However, retinyl ester levels doubled in the non-supplemented group immediately after the race (p < 0.001), whereas in the supplemented group similar high levels were observed not until 24 h post-racing (p < 0.001). The high levels of retinyl esters were paralleled to some extent by an increase in plasma triglyceride concentrations, which were significantly higher 24 h post-racing than immediately before (p < 0.001) and after exercise (p < 0.001) in both groups. The increase in retinyl ester concentrations might be indicative of their mobilization from liver and adipose tissue.
Thus, a sustained increased heart rate / blood flow stirs up more retinyl esters out of the liver and brings it into circulation.
A similar effect happens in women during pregnancy. Of course, it’s not just for 24 hours, rather it’s sustained for 7 or 8 months.
During pregnancy, the amount of blood pumped by the heart (cardiac output) increases by 30 to 50%. As cardiac output increases, the heart rate at rest speeds up from a normal prepregnancy rate of about 70 beats per minute to 80 or 90 beats per minute.
With that increased heart rate, more of the highly toxic retinyl esters are swept into circulation. Of course, the amount is probably proportional to the concentration already stored in their liver. Remember that retinol outside of the RBP can pass through cell membranes within about one millisecond. With that, there will definitely be a higher rate of conversion into retinoic acid. That prolonged elevated retinoic acid level would certainly explain the development of gestational diabetes. It would also explain other adverse accutane “side-effect” like conditions such as postpartum depression.
Quite interestingly, the same phenomenon has been observed in women recovering from breast cancer. Women who adopt a strenuous exercise regimen post cancer treatment have a much higher chance of their cancer recurring as opposed to women who only adopt a moderate exercise regimen. Likewise, emotional stress can have the same effect. This is why many people have reported that their first encounter with autoimmune diseases and cancer occurred shortly after a period of sustained emotional stress.
Intervention Studies
If this theory of vitamin A toxicity causing diabetes is correct then we might be able to confirm it with some intervention type studies using low vitamin A diets. There are indeed such studies. Let’s first consider Walter Kempner’s all rice and sugar diet. Kempner had his diabetic patients follow this diet for a period of up to 10 years and they had great results in reversing diabetes, obesity, and diabetic retinopathy.
Although some of his patients appear to have taken vitamin A supplements there’s no record of exactly what group those patients were in. Also, it’s very hard to know how much of it would have been absorbed on such an extremely low fat diet. Naturally, I think Kempner’s all rice and sugar diet is ridiculous and very dangerous. However, it completely contradicts the mainstream thinking on the role carbohydrates and sugar play in diabetes. None-the-less, it is very good evidence that we are on the right track here thinking that vitamin A toxicity is at the root cause of the disease.
Next, there’s another extreme diet from about the same era that had similar great results in reversing diabetes.
Blake Donaldson’s diet is the complete opposite of Kempner’s rice and sugar diet, yet it yields the same results with regards to reversing metabolic disease and diabetes. This “big fat steak” diet it’s now seeing a huge resurgence in popularity today. It’s called the “carnivore” diet. Why has the carnivore diet become so popular? Because it works! Like it or not, we have to look at the real-world results.
How can we explain these two diametrically opposed diets yielding effectively the same results in reversing diabetes? The common factor is that they are both inadvertently extremely low vitamin A diets. I think the carnivore diet is vastly superior to Kempner’s rice and sugar diet. But, in a way, when you combine these two dietary intervention studies they somewhat mutually exclude macro nutrients as being a major causative factor in diabetes. Therefore, that requires us to look deeper for mechanistic molecules. I say we go with putting the blame on the molecule who’s proven and very functional definition is one that destroys our stem cells. Yes, vitamin A is a stem cell killer.
Zinc – here it is yet again.
As with many enzymes, zinc is a key atom needed for the formation of insulin. Insulin is itself a protein based hormone.
The Structure of Insulin: Zinc is shown as the two magenta coloured spheres in the ribbon diagram on the right.
So, with background vitamin A toxicity putting a higher demand on the needed detoxification dehydrogenase enzymes, that could significantly reduce the availability of zinc needed for insulin production.
Could it be this simple?
For me at least, there’s no doubt that vitamin A toxicity is causing the diabetes and obesity epidemics. But, that’s just my own conclusion on it. With diabetes now being a major pandemic, it’s rather imperative that we find out. So, if you can, please help by tracking your A1C or blood glucose levels as you progress with this diet. You can then add more evidence (pro or con) to the case.
I am occasionally getting asked about the recovery time frame people might expect for themselves. Since everyone’s situation is unique, there are no easy and straightforward answers. All I can do is share what’s happened to me and from that information let people set their own expectations as to how long the road ahead might be. The only thing I can do is try to reassure people that I firmly believe it is at least on the right road.
Even with my own certainty about it, there are still a lot of unknowns. Firstly, there is a question of just how much tissue damage has occurred and how widespread it might be throughout the body. In the little bit I was able to determine about this, it looks like there can be 20% or more of tissue or organ atrophy/dysfunction before there are any real noticeable symptoms. Regarding the liver, the extent of the hidden damage can be much more significant. It can be somewhere around 80% damaged before people notice symptoms. In the context of blockage of coronary arteries, it might be as high as 50-80% before people notice it. Therefore, there could be a lot of damage that the body needs to repair and heal itself of. That’s just going to take a long time. Of course, there’s much more to the repair story. This type of damage is not as simple and as straight forward to recover from as recovering from say a wound or trauma-induced severe injury. This is not like a broken bone that usually heals in six weeks. What makes the chronic diseases so much more complicated is deeply-rooted in protein synthesis. After all, the disease itself is really the manifestation of defective protein synthesis. That’s what has caused the tissue to become damaged and malformed in the first place. Medical experts like to call this condition “metaplasia.” But, even though that’s a nice sophisticated sounding term, it does not mean that they understand even the first thing about the root cause of metaplasia.
Of course, I experienced this metaplasia often during my recovery period. It’s important to know that as time progressed, it became more and more localized, and then finally restricted to only a few small spots on my fingers. So, although I was making good and reasonably steady progress, it did take what seemed forever to fully redevelop well-formed, and regular and healthy skin again on my hands.
Okay, so let’s think about what’s really going on there. Why does it take so long to heal from the chronic diseases even after adopting a low vitamin A diet? The answer is partially found in this statement regarding the use of Isotretinoin, a.k.a. Accutane.
WARNING:Isotretinoin affects the entire body and can change not only the skin, but the entire body for the rest of a person’s life. This is why it is only approved for severe nodulocystic acne.
With a big warning label of: SERIOUS SIDE EFFECTS
The critical point here is that Accutane can, and often does, damage a person’s body permanently. Of course, since “Side effects are numerous and widespread, and affect almost all patients,” that damage is not a ridiculously so-called “side-effect” at all. Obviously, they are direct effects. And no, Accutane is not a “medicine” either, rather it’s a direct poison. And, no, doctors are not prescribing it for only “severe nodulocystic acne” either. Many are often prescribing it for mild acne too. It’s completely ridiculous to give this “drug” to any teenager, for any reason, ever.
But, for now, let’s just gloss over the fact that thousands of doctors are still routinely prescribing a drug for acne that has the well known “side-effect” direct-effect of permanently damaging a teenager’s body and often even inflicts brain damage on them too. What we are interested in understanding at this time is why and how does retinoic acid permanently damage the body. Why do so many people not fully recover from it after stopping its use, whereas, some others do?
The critical understanding needed to answer that question is found in the knowledge that the primary mechanism of retinoic acid’s magic action is that it causes “gene expressions.” Back in 1992, it was documented to be about 300 different gene expressions. The science has moved ahead a bit on it, and more modern literature now places the number at about 500 different gene expressions caused by retinoic acid (RA).
Next, we need to ask what are these gene expressions really? Of course, a major clue here is that RA is definitely documented as being a potentially deadly serious cytotoxin. And, since there are now more than 500 different gene expressions attributed to it, it should be self-evident. Has no one ever asked why are there so many different gene expressions? What’s the specific purpose of each one of them? It is also super critical to ask if RA is invoking these regulations of “gene expressions,” what molecule or enzyme is regulating that process? In other words, what governs and selects a particular one. For example, why does so-called gene expression #103 occur versus say gene expression #490? Of course, no one knows the answers to these questions. But, to any reasonably critical thinker, that number of 500 different gene expressions is the dead giveaway. They are not gene expressions at all. Rather clearly, they are merely random sites of where the RA molecule has bonded with the cell’s RNA and DNA and caused gene-damage. That’s right, they are indeed 500 different expressions of gene damage. Therefore, what we are really dealing with here are wide-spread RNA and DNA damage. So, for all the dermatologists who are still prescribing this wonder drug, that’s nice work guys, you are simply poisoning the RNA and DNA of your young patients.
Moving along here, and with that better understanding of the real mechanism of retinoic acid, we can ask what happens next? The short answer is metaplasia, inflammation and eventually so-called “autoimmunity” too. Of course, the body’s response is not always immediately noticeable. Retinoic acid picking off just a few cells at a time is not a big deal. In the development of the auto-immune diseases, it is usually a slow creeping process. It could take months, years, or even decades before someone has symptoms. But, we know that in the extreme case of Accutane use, it usually takes only about six months (depending on the dose and duration of the “treatment”).
There are at least two broad categories of the severity of the RNA and DNA damage going on. But, both manifest in defective protein synthesis. Cells are normally, and continuously, synthesizing proteins for cell repair, overall tissue maintenance, cellular replication, and for all kinds of other reasons. This is just a fundamental and necessary function of life. But, the supercritical detail we need to know here is that that the RNA and DNA is the cell’s protein weaving machinery. It’s very much like a super sophisticated biological loom that the cell uses to weave together all needed proteins. The generated proteins are beautifully and intricately structured molecules too.
The triple helix collagen protein molecule is an excellent example of one.
But, now with the retinoic acid molecule randomly stuck in the middle of the weaving machinery, the cell is going to be continually assembling defective proteins. Although defective, the cell is going to be diligently doing it over, and over, and for the rest of the cell’s life too. The cell is just doing the best it can manage. In one damage scenario, the generated proteins might be so severely malformed that it is just not usable at all.
In another scenario, the generated proteins may only be partially defective. Either way, the body is now trying to repair and maintain itself with faulty structured proteins. The tissue eventually develops metaplasia. And, that is the perverse and insidious mechanism as to how Accutane really “works.” It slowly wipes out the stem cells of the sebaceous glands of the skin, and many of them throughout the rest of the body too. So, that’s how it shrinks the sebaceous glands (and BTW often the testicles also, and sometimes it even results in the slow chemical castration of young men; that’s more real nice work guys).
And that’s how and why retinoic acid can permanently damage a person’s body for the rest of their life.
Therefore, even though we can adopt a low vitamin A diet, those DNA damaged cells still exist. How long they’ll last for depends on their host tissue and location. But, it could be going on for many years.
That’s probably not a very comforting thought. And, there’s even a bit more bad news here. Some of the defective proteins are going to be so malformed that they are going to appear to have come from a foreign species to the human body, or maybe even just foreign enough specifically to our own body. When that happens, the immune system is going to move in and attack the cells that are generating them, a.k.a. “auto-immunity.” I’ve already spent way too much time in ETFOH discussing this topic so I’ll just leave it at that.
With all of the above information, you can see why eliminating vitamin A from your diet is just the starting point in a recovery. It is not going to immediately, or even quickly, heal the body. All the existing RA damaged cells are still going to be perpetually assembling defective proteins. Thus, you could have on-going “metaplasia” in various tissues and organs for quite a long while.
But, I don’t want to paint too bleak of a picture here either. I have complete confidence in the human body and in its natural healing powers. I just want to set the expectation that it is going to take time to recover fully. In my personal experience, I was extremely sick too, and as about as sick as a person can be without dying, yet, I did recover from all of this mess. I made most of that recovery in about the first year. I was actually through the worst of it in about the first three or four months too. Of course, things rarely always work out in the first attempt. I foolishly thought that I should supplement with lutein and zeaxanthin. It didn’t hit me right away; instead it wasn’t until after six weeks into that supplementation I had realized my mistake. That little bit of carelessness was a huge setback, and it easily cost me at least another 6 months in more recovery time. I then more slowly made a complete recovery over the following three years. But, even just after the first year I was in pretty good shape and had nothing much to complain about. I expect younger people will recover faster.
Detox setbacks and symptoms
With that time expectation set, it would still be great if people just slowly yet progressively recover by adopting a vitamin A elimination diet. Although that is indeed sometimes happening, it is not happening for everyone. Some people have reported that they experienced an initial period of health improvement, and then they’ve moved into a phase where their condition and health gets far worse and even worse than before they started on the diet. Dr. Garrett Smith has called this a detox phase. I have a plausible hypothesis on why it’s happening. But, it’s just a hypothesis. So, please apply your own critical thinking to it.
I think what’s happening is that as the regular vitamin A serum levels start to decline, then just due to the mechanism of chemical equilibrium, more stored vitamin A is released from the liver. That’s just what we want to have happen right? Unfortunately, there’s a catch to it. There is a relative toxicity scale to the various forms of vitamin A. Obviously, retinol captured in the RBPs is not very toxic at all, next up is unwrapped retinol, and then it’s the retinyl esters, followed by retinoic acid. So, that storage form in the liver is actually quite toxic. And with it now being released faster than usual, people would experience its increased toxicity.
The following is from a 1981 report by Anthony R. Mawson and Gabriel I. Onor titled: Gout and Vitamin A Intoxication: Is There a Connection?
Retinyl esters react more randomly with the membranes of cells than the physiologically sequestered retinol bound in holo-RBP; hence, they are a major form of vitamin A toxicity.
Other sources back up and confirm this information.
Additionally, much of the liver’s retinyl esters are in the retinyl palmitate form, and that’s a more water-soluble molecule. Thus, that might explain why some people are experiencing foamy urine after being on a low vitamin A diet for a while.
Foamy Urine and leaking kidneys
Of course, it’s not normal to have protein leaking into the urine. It is a key marker for kidney disease. So, I don’t want to at all minimize these reports of foamy urine. It is definitely a serious concern. But this is not an ordinary situation for people to be in either. Therefore, let’s not jump to conclusions on it.
With that, and somewhat reluctantly, I now want to share my own account of being diagnosed with chronic kidney disease (CKD). It started way back in 2006 with a routine screening check for an insurance policy. The test had detected protein in my urine. Repeated tests by my GP over the following year revealed that my situation was worsening. A more comprehensive analysis showed that I was in trouble and I was referred to a specialist. A nephrologist. That was the first time I had even heard the term. Later I learned that the nephrons are the delicate structures in the kidneys that are responsible for filtering the blood and extracting water-soluble waste products into urine. Up until that time I had pretty much zero exposure to the medical sector, and I held doctors in high regard. Like most people, I felt these folks were the best of the best in science. Therefore, before seeing the specialist, I was not too concerned. After all, there’s been about a hundred years of advancement in modern medical science, so I thought that surely they’d be able to take care of me.
My appointment with the nephrologist didn’t go as expected, to say the least. Basically, I was sent to the nephrologist to have “the talk.” He was a nice young man, who appeared to be very knowledgeable.
He politely explained that actually, no, there was nothing he could do for me. He showed me the charts where they had plotted out my progressively increasing protein loss, with a nice regression curve fitted to it. He then told me that my condition had been detected early, and that I had about five years left, and that I should get my affairs in order. He told me to expect to be on dialysis in about the next two years. He went on to explain that dialysis is not a long term treatment, it just buys you some time. He also explained that things can get really ugly on dialysis and most patients just decide to stop it after two years, and they then die shortly after that. He went on and explained why I was not going to be a candidate for a transplant, and the odds of finding a donor were about the same as winning the lottery.
Very strangely, I was not too shocked by this information, and I wasn’t really upset by the news. I wasn’t being flippant about it either. I am just practical, and the news was what it was, and I would just have to deal with it. Yet, having two teenage boys, and knowing that I was not going to be around for them was really an unpleasant realization.
Next, here’s where the story gets really interesting, if not just wacky. Being the practical kind of guy that I am, and being very medically uninformed, I asked him, “What’s the big deal with losing protein anyways, why can’t I just eat an extra steak each week and make up for the loss?” He explained that the concern wasn’t that the protein was being lost, rather it was that the protein loss was a biomarker for the progressive breakdown and apparent self-destruction of the nephrons. He explained that medical science had suspected that additional protein in the diet might be stressing the kidneys, and it might actually be making the situation worse, or even accelerating the breakdown of the nephrons. He then went on and told me about a study he had just headed up to test this theory. It was a large study conducted between Canadian and UK researchers. They took 7,500 people with Chronic Kidney Disease and put them on a zero protein diet. He then said that it didn’t go very well, and I quote him: “we ended up killing most of them in three months.” Clearly, their “study” did not help these people at all; instead, it accelerated them into death.
I was stunned by what he had just told me. I could almost not believe what I had heard. I completely set aside my own grim diagnoses; it just didn’t matter to me after hearing that. I tried to remain calm, but my brain was racing ahead in trying to make sense of it. On the one hand, I thought good for him to be admitting this, but on the other hand, I had never met a self-confessed killer before, let alone a serial killer. I was really, and visibly, upset by this information. Maybe he thought the reality of my own diagnosis was starting to sink in, but that wasn’t at all the case. I was just getting angry about what he had told me.
Here’s the thing, I only have grade twelve biology, and maybe five undergraduate courses in chemistry, and a few in organic chemistry. But, what I do know is that there are about 50 trillion cells in the human body, and there are approximately 10 million cells that turn over every day. Every single one of those cells is built up by proteins. Protein is essential to their structure and functioning. Therefore, what they did was to take away the most basic building blocks of what these people really needed to maintain and potentially even heal their bodies.
How could modern medical doctors think that putting sick people on a zero protein diet was going to be viable? I mean, this is about as basic as it gets. I then thought about where do you get 7,500 study subjects from? Well, of course, it’s mostly from their GPs who refer them and enroll them in these studies. So, there would have been quite a few doctors involved in conducting and monitoring this study. How could all of these doctors have not raised serious concerns about their kidney patients being placed on a zero protein diet?
I then asked my nephrologist: “Why wouldn’t you have started with a 7 person, or even a 75 person, study just to be safe? Why start with such a large number of 7,500 people?” He went on and explained that I did not understand modern research, that it’s now all about “evidence-based medicine” and they needed to conduct these big studies to get a strong statistical significance in any finding. I retorted that even one dead person has a strong statistical significance to me.
I’ve subsequently learned that these “failed” studies are rarely published, even though they are usually taxpayer funded. They are quite often just swept under the rug and buried so to speak. However, I’ve never checked if this one was published or not.
I’m really not the type of person to jump to conclusions, but I had heard enough. I then asked him “Why do you even have a job?” What I really wanted to ask him was “Why aren’t you in jail?” I mean in any other field if you killed most of 7,500 people, you are going to be held accountable. I went on and asked, “If you can’t do anything for people, and you have no effective treatments, no cures, what’s the point of your job?” He explained that it was to plan and schedule people’s dialysis program. I stood up, thanked him for his time and told him to cross my name off his patient list, and that I would not be coming back. I told him I had no interest in his dialysis treatment, and that I would just let nature take its course with me. And that’s exactly what I did. Over the next few years, my health did get progressively worse. Even though my wife often asked me to go back, I never did.
To this day, I am still really bothered at how foolish their zero protein experiment was. I am shocked that this could have happened in Canada. It is something I might expect to have occurred in some third world banana republic. I can only hope that there were no children among the 7,500 people enrolled in that study. Still, I think it’s a shameful debacle. Even though I’ve subsequently learned that killing patients in studies like this is rather routine; there is no way I can accept it. There is something drastically wrong with medical science where this is allowed to go on. Killing people with gross incompetence is a crime. There is no way “doctors” should be getting a “pass” on it either. Not in the name of their pursuit of so-called “medical science,” or for any other reason.
By the end of 2013, my kidney function was severely declining. A few times I had blood in my urine, so I assumed that the end was near. Even with that, I wasn’t suffering too much. Ironically, learning about this nephrologist’s botched study was one of the best things to have happened to me. Because of that information, I had almost entirely checked out of the medical system. I had lost most of my trust in the system. And that was one of the best decisions that I have ever made.
But, the point of me relaying this story is not to go doctor bashing. Instead, it is to highlight just how little medical science truly knows about the human body. It’s also about how something so unbelievably basic can be overlooked or ignored by the experts. But, there’s a bunch of good news here too. Although having leaking protein from the kidneys is not normal, it is also not necessarily CKD either. It is just the body’s response to an extreme condition.
Most importantly CKD does not need to be chronic either, and that should be very good news for the now 30,000,000 people in the USA alone with progressive kidney disease. Additionally, being given a terminal diagnosis by the “experts” is not very meaningful either. Sure, in my case n=1, but I don’t give a hoot about their claim of needing large studies to prove some statistical significance. On the contrary, I think their reliance on some big “statistical significance” is a lazy cop-out for not using critical and logical thinking. In a way, it also rigs the system to where only big and well funded clinical organizations can do medical research. How convenient is that, huh? So, no, I’m not buying their nonsense, and n=1 can be hugely significant. All indications are that I’ve now made a full recovery from my CKD. I no longer have leaking protein.
Vitamin C
If there’s going to be more of the retinyl esters back flowing from the liver into serum, is there something else people can do to mitigate the harm? Unfortunately, I don’t have any great answers. But, I’ve since learned more about vitamin C. What’s interesting about vitamin C is that it appears to be only moderately beneficial when people are healthy. Conversely, where vitamin C really shines is when taken when people are sick. It is also reported to be very protective in the context of vitamin A toxicity. So much so, that I think, scurvy might just be misdiagnosed vitamin A toxicity. The reason that vitamin C plays such a critical role is that it facilitates the formation of collagen and bone rebuilding. These are two of the first tissues affected by vitamin A toxicity. Although vitamin C is not at all a direct antidote for vitamin A toxicity, it appears to play a critical role in accelerating the body’s repair process from it. Even though I had mentioned the need for vitamin C in my eBooks, I think I seriously underestimated its importance. Here’s a rather now famous news report about its powerful potential.
Ironically, the doctors in this case appear to do everything they can to not treat this guy with vitamin C. And, rather than being thrilled about having cured his cancer with vitamin C, it’s almost as if they were afraid to have anyone find out about it.
Salt
Likewise, a similar beneficial effect applies to salt intake. What I did not fully appreciate earlier was the importance of salt in the proper development of bile. Salt is needed to bind with the retinoids, and probably with other toxins too. In doing so, they can be more safely released from the liver into the bile. Without an ample salt supply, this process is going to be severely hampered. Here’s a snippet from the 1925 vitamin A research report that reflects the benefit of salt in reducing the severity of vitamin A toxicity.
TISSUE CHANGES FOLLOWING DEPRIVATION OF FAT SOLUBLE A VITAMIN.
BY S. BURT WOLBACH, M.D., AND PERCY R. HOWE, M.D. From the Department of Pathology, Harvard University Medical School, and the Forsyth Dental Infirmary, Boston. Received for publication, September 4, 1925
This mixture of inorganic salts was found by McCollum, Simmonds, and Becker to be adequate in the prevention and cure of a form of ophthalmia described by them, and which develops in rats supplied with fat-soluble A. It is interesting to note that Mori regards this form of ophthalmia as identical with that produced by deprivation of fat-soluble A, but his very brief description of the pathology does not support this conclusion.
Ironically, our more modern medical advice has for a long time now vilified salt. The “experts” have been warning people about consuming too much of it for fear of the risk it might have in thickening the blood and subsequently causing high blood pressure. But, they’ve entirely ignored salt’s very long history of its beneficial role in the human diet. Go figure?
Protein
At the risk of being overly repetitive, I just want to make sure that anyone who adopts a low vitamin A diet includes an ample amount of protein. An all-rice diet, or an all-potato diet, is definitely not going to cut it. It would also be very dangerous too. Personally, I believe that animal sources of protein are going to be better when adopting a low vitamin A diet. But, that’s just my opinion. As always, please apply your own good judgment on it.
The Subclinical saturation & Toxicity of retinol & retinoic acid
Introduction
This document investigates the root cause, and connection between the seemingly disparate diseases of Eczema, Crohn’s and Alzheimer’s disease.
There are a bunch of even more seemingly disparate pieces of evidence that I present to make this connection. These can be thought of as pieces of a puzzle if you like. Once connected, they reveal a pretty clear picture. Or, if you prefer, consider them to be clues that enable us to track down a notorious serial killer.
This document is not intended to be an scientific publication. It is an mix of theory, evidence, and my own personal account and observations in dealing with one of these diseases.
Even though this is a very long, and rambling document, if you have an autoimmune disease, or you are genuinely interested in this topic, then I think it is worth your time to read all of this. If at any point while reading this you think something is wrong, or that this can’t be correct, please leave a comment as to why you think so. Also, please understand that I am presenting this as a theory. It could be wrong, and completely wrong. It could be right, or only partially right. I am completely, and totally open minded about this. However, the preponderance of evidence that I have found is indeed pointing in this direction.
Autoimmune diseases and Alzheimer’s are not trivial topics. This is complicated, and it requires a lot of evidence.
The evidence topics (in no particular order) include:
WHO and pregnant women in India
Vitamin A
Food
Japanese Skin Rejuvenation Therapy
Crohn’s Disease
Eczema
Hair follicles
Government Regulations
Autism
Charles Darwin
Hashimoto’s and the ⅓ missing eyebrows
National Institute of Health
Pickled Herring
Socioeconomic status
Fatty Liver Disease
Exponential decline curves
Winter Air
Mucosal Calcinosis
A man named John
An Acne Drug
Symmetry and randomness
The Koebner phenomenon
The sebaceous gland
Thresholds and tipping points
The closure of the Atlantic Cod fishery
The border between Finland and Russia
Kids
Chile
Steroid creams
Anorexia
Spontaneous Bone fractures
Retinal Neurodegeneration
Fluorescence
Handwashing dishes
Canada
North South ocean temperature gradients
An incredibly well known toxin
Age 20ish
Band Aids
Fortified Milk
I’ve highlighted what I think are the most important pieces of evidence. What are the connections between all of these? If we can answer this, then I think we can solve the mystery.
With all of these topics to discuss; this is going to be a very long read. Hopefully, there is a bit of intrigue raised here.
Although I am using intrigue, and puzzle metaphors; I do take this to be deadly serious. This is no game. Alzheimer’s and Autoimmune are the biggest diseases of our time. They are killing millions of people, and destroying the lives of 10’s of millions of others. Statistically speaking, every 60 seconds another person in North America is being diagnosed with Alzheimer’s disease. That is effectively a death sentence. Consider this; right now in Canada 48% of men, and 67% of women by age 85 have Alzheimer’s or dementia. If you are lucky enough to live to be 105, then the probability of having Alzheimer’s is 95%.
Not too long ago, autoimmune diseases (all of them) were actually very rare. Alzheimer’s was a very rare disease too. Nearly all of a sudden; that has changed. We are in the midst of a raging epidemic of these diseases. We could actually even be at the early stages of that epidemic. Something is hugely wrong.
Approximately every 30 seconds another person is now being diagnosed with an Autoimmune disease. That is effectively a life sentence of future misery.
So, this is my attempt at cracking the code on this puzzle. I’ve also just recently joined the illustrious autoimmune club. Last year I was diagnosed with Eczema. It was just a rash; but I did not like it. I did not like it one little bit. That has put me on a bit of a mission to try to solve it. I have no medical experience whatsoever. I am just a guy with a rash. So, how does a guy trying to solve a rash stumble upon all of this? It was by conducting a very simple experiment.
OK, let’s dig in, and get started.
Here are some charts that I put together revealing what I think is an amazing connection. These charts are key pieces of evidence needed to solve this puzzle. Please do not gloss over it. Look at it very, very carefully. Not to overstate it; but these are incredibly important evidence. Please understand that these charts are revealing some major new clues as to the root cause of a major Autoimmune disease, and directly correlates that disease with Alzheimer’s disease. Also, these charts are original, they are not copied from anywhere. They are showing reliable; scientifically published data.
If we can understand what happened here; and fully understand what the connections are, then I think we will uncover the root cause(s) of these diseases. If we can solve one of these diseases; we may be able to solve the other. How hard can it be to crack the code on one of these? Click the chart to zoom in if you want a better view.
This is data from Atlantic Canada from between 1996 and 2011. The top line is Crohn’s disease incidence rates in Nova Scotia, and the others are Alzheimer’s mortality rates in the Atlantic provinces.
A remarkable ~35% drop in Crohn’s disease over this time period (1996-2009)
A stunning ~50% drop in Alzheimer’s mortality over this time period ( 2000-2011)
These two trend lines for Crohn’s and Alzheimer’s disease are nearly parallel
Western Canada has no such decline (both are increasing in Alberta)
Most of the rest of the world has no such decline in either of these diseases.
Here is the Canadian Alzheimer’s Data; from the East to West coast provinces. That east to west ordering is very important. Please look at these numbers very, very carefully. What do they tell us? You can maybe visualize a big arrow from the top left to the bottom right.
Alzheimer’s disease Age-standardized mortality rate per 100,000 population, Both sexes
Alzheimer’s disease Age-standardized mortality rate per 100,000 population, Both sexes
Here is a chart showing the Alzheimer’s mortality rates in most of the other Canadian provinces.
The key observations here are:
The decline rate in Canada’s western most provinces is nearly zero. In the year 2000, the Atlantic Provinces where at least 1.5 to 2 TIMES the rate of BC, and Alberta.
ALL the Atlantic coast provinces are all at the top of the chart. All have clearly significantly higher rates than the rest of Canada.
The significantly declining rates over this time period; but particularly so in the Atlantic Provinces.
The slope of the regression lines on NL, NB are much steeper than that of BC, and AB. The BC regression line is almost flat.
The Nova Scotia rate changes are a bit different than the other Atlantic Provinces.
By the year 2011, the rate of most of the Atlantic provinces is cut in half, and is approaching the same rates for western Canada
Once again, most of the rest of the world has no such dramatic decline in the rates of these two diseases.
What does this tell us? It tells us; with crystal clear clarity, that these are environmentally induced diseases. There has been a pervasive environmental change in Atlantic Canada to cause these significant declines. I suggest that there is no other logical conclusion.
The charts shown above include quite a few curves, and end up looking a bit cluttered. Here is a chart showing just the Alzheimer’s rates in Newfoundland and the Crohn’s rate in Nova Scotia.
I picked these two curves just to emphasize the significant trend here. But, no matter, all the Atlantic province curves are similar. The decline rates in these two seemingly completely disparate diseases are tracking each other very closely. I think that there is just no way that the underlying cause of these two diseases is not indeed related. For me, on one hand this is remarkable data. But, on the other hand, based upon my battle with Eczema, it is exactly what I suspected. After-all; I did not just randomly think to go and look for possible correlations between Crohn’s and Alzheimer’s. You might be asking yourself; “what the heck is this guy talking about; a connection between Crohn’s, Eczema and Alzheimer’s?”. Well, I believe that indeed there is. They are directly related. They share the same sinister parent. If you can take the time to read this entire document; I think the reasons why will become completely clear.
What happened in around 1996? Canada closed the Atlantic Cod fishery in 1993. So, there is something fishy about this story. Here is something else that’s fishy. The Alzheimer’s rate directly across the Finland – Russian Border.
Finland is 22 TIMES higher. That is not a typo. Finland also has one of the highest rates of Eczema in the world. Sweden and Denmark have some of the highest rates of Crohn’s disease in the world. What does this tell us? Once again, if we can understand why this difference is happening, we are well on our way to solving the mystery. A partial clue is the Finns eat lots of fish, and fish oils; whereas their Russian neighbors do not. But, this story is not about fish! It is about what is hidden inside the fish.
Here’s a bit of trivia. Consider the two cod fish shown below. They are the exact same species; the same age, size, taste, and smell. The only difference is one came from the West coast, and the other from the East coast of Canada.
What is different about these two fish? The difference is that the Atlantic Cod has 10 TIMES the level of vitamin A compared to the Pacific Cod. It appears to be the same fish; yet it’s 10 times higher in vitamin A. Why is that?
My journey, the other evidence, and connecting the puzzle pieces.
Okay, let’s dig into the science of all of this. The basic premise to this theory is that Eczema, Crohn’s and some other common autoimmune diseases are caused by being in a chronic state of elevated levels of retinol, retinoic acid, and possibly the carotenoid vitamin A precursors.
However, this is not the same as acute or chronic vitamin A toxicity as documented in the medical literature. No, almost not at all. Rather it is a sub-clinical poisoning that develops slowly over years; and possibly even over decades. There is a level of toxicity way below the documented acute or chronic vitamin A toxicity cases; yet the end results are far more devastating. Autoimmune diseases are actually auto-poisonings! So is Alzheimer’s.
The World Health Organization and pregnant women in India
A key piece of information for me was reading a report of a WHO program conducted in India; where they were pre-dosing pregnant women with 400,000 UI of vitamin A in one dose.
They were monitoring the blood serum in some of these women as they digested this dose. An incidental comment in the report was that they were amazed at just how fast the body removed the vitamin A dose from the serum. Of course this dose was quickly absorbed by the liver and stored away. The time between digestion and absorption was very brief (they did not numerically quantify it).
Okay, that’s fine. There is no comment in the report of a follow up study as to how many birth defects this program may have caused. Nevertheless, this was a critical point for me in understanding what might be going on. It means the body really does not want unbond Vitamin A in the serum; nearly not at all. Fine, and not surprising; since this is what is expected to happen in a normal healthy person. But, there is a limit on how much the body can physically store.
Exactly what happens when we consume too much Vitamin A
If you are a researcher; or a medical person, then the obvious question for you is what is going to happen once the body approaches or reaches this storage limit? We all need to know the exact and correct answer to this question. There can be no glossing over this. It is a critically important question; since vitamin A is in nearly all foods.
The food supply in North America is hugely supplemented with it too. It is also a critical question because most people in the Western / Industrialized world are going to eventually get into this state. It is more or less a mathematical certainty. What’s going to happen once the body nears storage saturation for vitamin A?
I think it is obvious that since the liver can no longer quickly absorb and store this intake; it is going to remain in the serum longer. This results in sporadic or chronic excessive vitamin A levels that surges and overwhelms the normal and dedicated storage function. Other systems and organs are now attempting to contain this overflow. It is also not quite this straight forward.
Consider yourself getting into this state. You’ve just gotten yourself into a vitamin A toxicity state. You are going to become sick, and very sick over time. All kinds of horrible things are going to start happening. There is no antidote as far as I know. You’ve now fallen through an almost one way trapdoor.
If your average daily intake is more than your body’s daily usage, then it is more or less inevitable. If you indulge just a little bit on too much milk, dairy, eggs, certain fish etc or any of the vitamin A precursors, then this is going to happen much sooner. If you supplement with cod liver oil, or a vitamin A supplement, or any vitamin A derivative; it is going to be much, much sooner. It could be in your twenties or teens or even at birth! It is also going to depend a bit on what you consume that vitamin A with.
Since your liver can no longer protect you; your other organs and immune system is going to go into action and attempt to deal with has now become a horrible toxin. Every mcg of consumption could now be toxic to us. You now have an autoimmune disease. You are now in the same group as about 30+ million other people in North America. Welcome to the club.
These diseases are really the result of non liver accumulation of this potential toxin.
What is happening here is the other organs, such as the skin, lungs, kidneys, GI tract, joints are accumulating too much Vitamin A. Although these organs & tissues are capable of storing or accumulating vitamin A; this is an extraordinary defensive measure taken by the body to locally store excessive amounts. This should not normally be happening. This would have rarely happened during the evolution of humans.
Of course, we actually don’t have to speculate what is going to happen when we reach elevated storage levels. It is incredibly well documented in the scientific and medical literature. More on that a bit later.
Eczema and making the initial Connection
When I made my initial recovery from eczema using my vitamin A elimination diet; some other remarkable things happened to me. All kinds of other subtle, and not so subtle, negative health symptoms that I was experiencing quickly went away too. These were symptoms that had slowly developed over a 5-10 year period; so slowly that I had mistakenly assumed they were just a normal part of aging. So, that was a pleasant surprise to have them magically go away. Moreover, it became abundantly clear to me that I had more or less turned off what my doctor told me was an autoimmune disease. Most importantly, it was perfectly clear to me that eczema was just a symptom (a very nasty one) of the real underlying cause. Unfortunately, this underlying cause is hugely more serious than the eczema skin condition itself.
Therefore, the most important thing to really understand about eczema is that it is not just a rash. It is much, much more than a rash. It can also be fatal in an indirect way.
It is actually the skin being dissolved from the inside out. You need to really understand and appreciate that last sentence. The word dissolved is a precise, and carefully chosen word. It is not an exaggeration or an analogy.
How do I know the skin is being dissolved? Because I have watched it happen, in real time, on the backs of my own hands and fingers, under my microscope. I have done so at least six times. An analogy would be to watch a sugar cube dissolve in water in real time.
Even at just 30x I can see what I am calling the matrix of the skin (the collagen?) more or less disintegrate. Depending upon the severity of the inflammation, this process can take less than 5 minutes to burn through to the top layer of the skin. It often burns the top layer right off. It is super important to know that this is coming from inside the skin. It is not from the surface in. If the top layer of the skin does not dissolve; it has hundreds of little craters burned into it. Paradoxically, with the inflammation the skin can subsequently become much thicker.
KEY EVIDENCE: Never let the Skin Air Dry: it will make your autoimmune disease get worse
Of course this is not just my observation. The very common recommendation from medical people and other people with eczema is to dry yourself off very carefully after a bath or shower. The advice is:
“Blot dry with a towel (rather than rubbing), and apply a moisturizing cream from head to toe (focusing on problem areas) within 3 minutes of getting out of the bath or shower, while the skin is still moist. If the skin is allowed to air-dry before the moisturizer is applied, the eczema could get worse.”
Why is this? Well for two reasons. Firstly, it is because the skin in affected areas is so incredibly thin, thinner than rice paper thin, or disintegrating, that if you rub it the least little bit you’ll rub it right off. The skin can be so thin, that it has no structural integrity left to it. At this point it can be more like a thin layer of mush.
Of course, if you do rub it off; it is both a bit more painful, and you now expose yourself to the risk of bacterial infections. Once again, this thinning of the skin has happened from the inside out. The top layer of the skin has been dissolved away. I think for most people, if they were to look at eczema affected skin during a flare-up under a 30x microscope they would be shocked. It is actually an amazing amount of destruction going on. There are hundreds of little pockets of skin per square centimeter that are completely burned out. The hair can be completely burned off at the skin surface level too. Unfortunately, I don’t have a camera attachment for my microscope; so I don’t have a 30x picture to share. I do have pictures from a regular camera share here.
The second, and other huge clue here is this : “If the skin is allowed to air-dry before the moisturizer is applied, the eczema could get worse.”
I can’t tell you how many different places I’ve seen this same statement. This is like a universal observation with eczema. Now, why does letting the skin air-dry cause an autoimmune disease to get worse? The short answer is that the last thing you want to happen is for the body’s natural mechanism for moisturizing the skin to go into effect. The longer answer is just a few pages below; and you are probably not going to like it.
So what about this dissolving, crumbling skin? What chemical is capable of doing this to the skin? Retinoic acid of course.
Vitamin A acid peels
You can actually get prescription cosmetic applications to accomplish exactly this. They are called Vitamin A acid peels. There are various products on the market. They dissolve the top layer of dead skin cells to expose the newer deeper layers, and promote skin turnover. Similar products are available as an acne treatment. Nice for them I guess. But, people with eczema are effectively applying a similar acid peel from the inside out. This might sound like something out of a horror novel. But, it is not. It is exactly what is happening.
Although the reference to Vitamin A acid peels might be something that a lot of people are aware of, or can directly relate to, it is not very strong evidence scientifically speaking.
Key Evidence – Japanese Skin Rejuvenation Therapy
Let’s look at some more scientifically based evidence. Here’s a great collection of recent research papers on the topic of Retinoic Acid.
Chapter 6: Tretinoin-cyclodextrin Complex in Skin Rejuvenation Therapy
Authors:Cheng, Li-Hong, Ito, Yuto; Osaka University, et al.
ISBN 978-1-62100-597-1
Tretinoin is all-trans-retinoic acid ( let’s use the ATRA abbreviation).
In a nutshell, what they are researching is the development of the topical application of ATRA (retinoic acid) to reduce the effects of chronological and or photo-aging of the skin.
They document that ATRA will induce improved skin turnover, and ultimately the thickening of the collagen. However, when applied directly, and topically, they report that patients frequently experience inflammation, redness, scaling, itching, and burning, and desquamation. Okay, it appears that they are directly inducing the eczema skin condition we all consider to be an autoimmune disease.
But, if the patient can tolerate these conditions for a while, then after stopping treatment there is a subsequent thickening of the collagen. This is exactly the same condition observed with eczema; after the skin becomes inflamed, it usually turns much thicker. Overall, this now sounds like the textbook description of Eczema.
The authors describe the mechanism as: “The phenomena occur because Tretinoin releases heparin-binding EGF-like growth factor (HB-EGF), which enhances the proliferation of basal cells”.
This little detail of the EGF-like growth factor being released is a very important one to remember.
ATRA works in thickening the collagen, but they need to directly deliver it deeper into the dermo skin layer, without first inflaming the epidermis, the outermost layer of skin. They adopt some rather novel ways of bypassing the epidermis; and getting the ATRA deeper into the skin. I will try to contact the authors to see if they can provide photos of the inflamed skin they were inducing.
There are many more papers providing scientific evidence that retinoic acid may be the culprit here. Retinoic Acid has been used in dermatology since 1959. It has been used to treat many skin related diseases such as acne, ichthyosis, psoriasis and others. However, the complication of skin inflammation leads to the interruption of treatment by many users.
Here is another research paper on a similar topic:
Chapter 10: ALTERNATIVES TO REDUCE THE TOPICAL RETINOIC ACID-INDUCED SKIN IRRITATIONA.
Authors: Castro and L.A.M. Ferreria of the Federal University of Minas Gerais, Brazil
The authors discuss several approaches for addressing the concerns of patients attempting to use Retinoic Acid treatments topically.
The key points in this paper are the documented side-effects of skin irritation that include: erythema (redness), dryness, peeling, and scaling and the breakdown of the skin’s barrier function.
Well; are these not very interesting side-effects? This is once again like the textbook description of Eczema.
What is really interesting about this paper is that they document the exact process at the cellular level as to why this happens. The retinoic acid causes the gene expression leading to the immune inflammatory response. This is a fantastic paper in many ways. It documents the nuclear hormone receptors that bind to the RAL and the RAL isoforms, They also document that these same nuclear receptors accept steroid and vitamin D. That’s really, really interesting to me.
This paper also points out the the overload of retinoic acid is indeed the direct cause of the skin irritation, inflammation, erythema, dryness, peeling, and scaling condition. It is a bit odd to me that they call these conditions “side-effects” when they know the exact cause is the topical application of the RAL. Maybe they should have termed these the “direct skin response effects”. Fortunately, those documented side-effects are once again pretty clear evidence that RAL could be the culprit in at least causing the Eczema skin condition.
Now we have this solid scientific evidence that Retinoic Acid does directly cause the Eczema condition. It is completely, and easily, repeatable by anyone. This repeatability is the foundation of the scientific method. But, I am personally not volunteering.
Of course, in these papers the retinoic acid is being applied topically. So, is it possible that the eczema skin condition (the autoimmune one) is caused by retinoic acid internally building up in the skin? Of course it is. This exact accumulation process is documented to happen in the adipose tissue, the sebaceous glands, and elsewhere.
But, where is that retinoic acid coming from? The vitamin A in our food is mostly in either the Retinol or the Retinal forms. Where and when does this conversion take place in the body?
From these two sources, it is clear to see that the body is going to convert excess Vitamin A (retinol) to Retinoic Acid. It is going to happen in the intestine, and at the cell levels in other tissues.
Retinol is metabolized to retinoic acid in normal cells.
At the cellular level, the normal pathway of delivery is for the liver to release retinol bound to, and contained within a retinol-binding protein (RBP). The retinol-binding protein facilitates the safe transport of the retinol within the blood plasma.
The cell has a surface receptor for this binding complex, and absorbs it via that receptor. From there the cell unbinds it, and metabolizes the retinol and converts it to retinoic acid. That retinoic acid then passes into the nucleus and is used for gene expressions, and subsequent generations of proteins. The gene expression can produce cytokines. The cytokines are signaling proteins, and are released by the cell. Some particular cytokines will invoke an immune response.
However, the cell also has surface receptors for unbound retinol. Therefore, unbound retinol can also pass through the cell membrane into the cytoplasm. From there; it probably follows the same path of conversion into retinoic acid, and the subsequent generation of cytokines. To me, it appears that excess plasma retinol is going to bypass the cell’s self-regulation mechanism for the generation of retinoic acid. Therefore, if I am understanding this correctly, it looks like this:
Excess retinol ⇒ absorbed into the cell ⇒ cell converts to retinoic acid ⇒ cell generates cytokines ⇒ immune cells respond ⇒ attacks the cell ⇒ inflammation ⇒ cell’s destruction ⇒ growth hormone released.
Therefore, it is not quite auto-immune; since we are indeed inducing it to happen. But, if we look at it at just a point in time; it sure appears to be auto-immune. We could also be training the immune system to wrongly respond in the future too; and without the presence of excess retinol. I don’t know.
Nevertheless, it is not “auto” in the sense of it happening automatically, randomly, and defectively. No, it is not random, and there is indeed a reason it happens. People don’t get these diseases just because of bad luck. Physical events always happen for a reason. That is just a fundamental law of science. So, I’d sure like to propose that we drop this silly notion of “Auto” immune diseases. We just do not understand the reason and process; but it is not magically “Auto”. What we are really seeing is Immune related diseases of “yet unknown” causes. If we all buy into this “Auto” thinking; then this may never get solved. Let’s see if we can get closer to understanding the real root cause(s).
The conversion from retinol to retinoic acid is going to happen a lot more in people with elevated tissue storage and even slightly elevated plasma levels of unbound retinol.
In normal healthy people, regular vitamin A consumption should mostly be stored, and stored very quickly, and efficiently by the liver.
The authors of the 2006 Toxic effects of Vitamin A report state: “Hepatic storage of vitamin A will continue until a pathologic liver condition develops”.
But, clearly there is a physical limit to this storage. Therefore, I think we can safely say: “Pathologic conditions develop once the Hepatic storage is exceeded”. Of course, this is not some thin line, or single threshold, that is crossed over. It is variable; and a variable over time.
So, where the heck is all this vitamin A coming from, in what appears to be normal people, on what we think are normal diets? It’s in all of our food!
This same chemical, or its precursor, is literally in nearly every food on the planet; in one form or another. Is eczema really an autoimmune disease?
What does this have to do with Crohn’s disease? Everything. I think Crohn’s / IBD is effectively eczema of the GI tract.
The suspected connection between Crohn’s / IBD and Eczema
When I first encountered Eczema; I had no understanding whatsoever about autoimmune diseases. However, it was not long before it came very clear that the common theme between all of them is inflammation. Depending on the body location of the worst of the inflammation, it gets a distinct medical name. To an outsider; it’s like why do we bother with all the separate names? Why don’t we just call them the same thing? Inflammation of tissue X. These diseases also share a large set of other amazingly common symptoms.
Would it not be truly amazing if most of them were being caused by the same thing? What’s causing all this inflammation?
Firstly, I think I’ve proven with my food experiment that Eczema is actually the result of a subclinical toxicity of vitamin A. This toxicity is clearly capable of not only burning holes in the skin, it is capable of literally burning the skin right off in extreme cases. This inflamed skin condition is occurring, to varying degrees, in at least 10 million people in North America at this very moment. And almost everyone controls it with steroid cream treatments.
There is no doubt in my mind that this same process is capable of burning holes (ulcers) in the GI tract, or anywhere else in the body for that matter.
Secondly, there are a bunch of other similarities. In both these diseases people experience periods of flare-ups. In both these diseases there can be extended periods of remission. In both diseases there is inflammation and tissue being destroyed. At a certain age, both diseases are considered chronic, with no real known cause, and no cure; just treatment. Both are considered to be autoimmune diseases. Both diseases use steroids as a treatment. Both these diseases have seen a doubling in incidence rates over the last 15 years or so. Both diseases are not modern day diseases. Eczema was well documented 200 years ago. Crohn’s disease was first documented some 90 years ago. No doubt it was occurring before this time too.
Both diseases are considered chronic inflammatory disorders where the symptoms can range from mild to severe. In both diseases tissue can be turned thick and leather like with inflammation.
Both these diseases affect young, and what should otherwise be healthy, people. In both these diseases there is a significant jump in incidence rates starting at about age 50. With Crohn’s there is a big jump in incidence rates around age 20. This 20ish number is another super important clue.
I think the only really big difference between these two diseases is just the body location where the destruction takes place. Eczema is on the external skin, and most often on the face and hands. Crohn’s / IBD is in the GI tract; the internal skin.
The Vitamin A Connection and the Subclinical Toxicity of it.
The official information from the National Institute of Health states that Vitamin A IS A DIRECT TOXIN at high doses.
We need to understand three very important facts:
Vitamin A is a toxin
The body stores this potential toxin
The body has a fixed capacity for storing it, and therefore, a limited ability to protect you from this potential toxin.
It is no secret that Vitamin A can be a serious toxin. This is well established, and abundantly documented. But, if there was ever a case of too much of a good thing being a bad thing, this is it. What about this “at high doses” part? From an engineer’s point of view, since the body stores this substance:
High Doses EQUALS the SUM of many small doses
Now, let’s get to know this villain a little bit better.
“Vitamin A is a retinoid and a fat-soluble vitamin that is commonly found in eggs, milk and liver and in the form of provitamin A in carotenoids in fresh fruits and vegetables particularly those with red, orange or yellow color. … and (cod liver oil)
Hepatotoxicity
Normal doses of vitamin A are not associated with liver injury or liver test abnormalities, but higher doses (generally more than 40,000 IU daily, ~12,000 μg) can be toxic. Acute toxicity is caused by a single or a few repeated very high doses (generally >100 times the RDA), arising within days to weeks with a typical symptom complex of severe headache, nausea, vertigo, blurred vision, muscle aches and lack of coordination, followed by skin desquamation and alopecia.
…
Chronic hypervitaminosis A usually arises 3 months to many years after starting moderately high levels of vitamin A (generally 10 times the RDA) and is marked by dry skin, cheilosis, gingivitis, muscle and joint pains, fatigue, mental dullness, depression and liver test abnormalities.
Mechanism of Injury
Vitamin A in high doses is a direct toxin. Excess vitamin A is stored in stellate cells in the liver and accumulation can lead to their activation and hypertrophy, excess collagen production, fibrosis and liver injury. The toxicity is dose-related and can be reproduced in animal models.”
How bad can this villain get?
High intake of the preformed types of Vitamin A are associated with toxicity, and can cause nausea, dizziness, elevated intracranial pressure (pressure around the brain), headaches, coma and death. High vitamin A levels during pregnancy are associated with birth defects.
The simple answer is; it can kill you! The more complex answer is it can first painfully destroy your body for decades, and then kill you.
Now, just like most villains; this one has a good side. At one level, it is not a villain at all. It is a critical substance for the human body. At the right level, it is not only harmless, it is essential for health. So, it is a double edge sword. It is also very, very tricky balance. It is not just how much you consume; I think it is going to depend upon what foods you consume it with.
Basically, the liver is the body’s primary storage organ for vitamin A, and the storage capacity can become more or less saturated, or maxed out. The skin and fat are secondary storage locations. If we have one of these diseases, then effectively, the body can no longer protect us from what is now a toxin. This substance is also in nearly all foods. Once we’ve maxed out our liver’s storage capacity; we are in serious danger. We’ve defeated our body’s primary defense mechanism from this potential toxin. Our immune system, and the skin are now attempting to deal with it. What happens now? If we consume just a little bit of vitamin A, it keeps the inflammation going. If we consume a bit more vitamin A, we experience a flare up and that burns holes in our tissue / organs. But, this is not some instantaneous event. It is of course more complicated, and the declining rates of absorption are what is really important. Here is a sketch as to what I think is happening.
If you are thinking, OK, great to know, I’ll just go low on foods that contain vitamin A. No, sadly, it is not that easy. Your liver is now maxed out; and maybe so is your skin. That vitamin A in your liver is not going anywhere fast, or soon. It is more or less trapped there ( to protect you from it, and to use it when needed). The vitamin A stuck in your skin, and other organs is trapped there for even longer; possibly much, much longer. Moreover, there are other artifacts from the immune response, such as cytokines and antibodies, stuck in your skin too.
Now, this is a very tricky, and delicate situation. If you surge your vitamin A intake even slightly beyond your body’s vastly diminished ability to safely absorb and store it; you are in big trouble. Moreover, my own experiment is also leading me to believe it is not just vitamin A, but maybe also carotenoids. Carotenoids are what are known as vitamin A precursors, and are found in brightly colored fruits and vegetables. Carotenoids are also used to make most foods colors. I think it is even more tricky, because it may depend upon what foods you consume vitamin A with. If you consume it with fats; it may bypass any attempt by the liver to store it. Rather, it may go directly to other storage locations.
If you have truly overwhelmed your liver’s storage capacity, then you probably need to go to near zero consumption of vitamin A for a while. The catch here is that nearly all foods contain at least some vitamin A, or carotenoids. Now every molecule counts. You also cannot consume any coconut oils either; based upon my own experimental evidence. I think that the coconut oils act as emulsifiers for retinol and carry it around the body.
People from the medical community will probably quickly challenge this entire theory of sub-clinical toxicity with this vitamin. They might take the position that there is no way millions of people are actually getting into a toxicity state. Well, let’s investigate this and see.
Matching Up Theory with The Facts
Now, let’s look at the symptoms of Vitamin A toxicity, and compare those with Crohn’s disease. But, just like with eczema, it is important to look at all the ancillary symptoms of Crohn’s disease, and not just the primary one of inflammation and tissue destruction. We need to take a step back from focusing on the primary symptom, and look at the bigger picture. Then the situation becomes clearer.
followed by skin desquamation and alopecia (hair loss)
dry skin
cheilosis (fissures in the corners of the mouth)
gingivitis
muscle and joint pains
fatigue, mental dullness
depression
Let’s match up some of these with those documented for Crohn’s
Vitamin A Toxicity (aka poisoning)
Crohn’s Symptoms
skin desquamation
skin rashes; and ulcers in the GI tract
cheilosis (fissures in the corners of the mouth)
anal fissures ??
fatigue
fatigue
abdominal pain
abdominal pain
nausea
Nausea
vomiting
Vomiting in some cases
vertigo, mental dullness
?? (please help if you know)
severe headache
headaches
bone pain
Joint pain, symptoms of arthritis
alopecia (hair loss)
alopecia (hair loss)
mouth ulcers
mouth ulcers
gingivitis
osteoporosis?
blurred vision
blurred vision
respiratory infection
no ??
confusion
?? (please help if you know)
sensitivity to sunlight
no ??
depression
Depression
It is not a perfect match; but there are quite a few shared symptoms. Some really key ones for me are mouth ulcers (canker sores), fatigue, and blurred vision.
I had these symptoms well before any sign of my eczema conditions. I had mouth ulcers (just small blisters on the insides of my cheeks) occurring off and on in the year or so before my first incidence with eczema. I had no idea what was causing them. They were not painful at all. Since I’ve been on my vitamin A elimination diet, I have not had a single recurrence, not one. They are completely gone.
Fatigue:
Severe fatigue is a documented symptom of Crohn’s, Lupus, and of course other autoimmune diseases.
I experienced severe fatigue too in the year leading up to my first eczema symptoms. I was needing 12 hours of sleep a day. Strangely, even that amount of sleep was not very helpful. I was still just barely dragging through the day. It was chronic; almost unrelenting fatigue that lasted close to a full year. I was also trying to get mid afternoon naps. Three weeks after adopting a very low vitamin A diet; all of the fatigue completely vanished. I am not talking about just a significant improvement. It was more like a 100% improvement. I now have absolutely no fatigue at all. It is completely gone. I now need only about 6-7 hours of sleep; and am totally refreshed and alert in the mornings. I have no mid afternoon low points at all. This in itself should be considered remarkable. I can’t overstate just how completely resolved my fatigue symptoms are. Even when I went back into slight flare up states with the eczema skin condition; the fatigue remained completely resolved.
Joint Pain and Body Stiffness:
Like fatigue; I was experiencing some significant joint pain, and body stiffness leading up to my eczema symptoms. This actually started back about 10 years earlier. It was very, very slowly getting worse. I assumed that the joint pain and body stiffness were just a normal part of aging (who doesn’t think this?). The body stiffness had become quite noticeably worse in the year prior to my eczema experiences. Within four weeks of my vitamin A elimination diet, those symptoms completely vanished too. I mean completely, totally gone. When I get out of bed in the mornings, there is no stiffness whatsoever. However, unlike with the fatigue, when I went back into slight flare up states with the eczema skin condition; a very slight amount of stiffness returned. That very slight regression only lasted for a day or two and has been gone ever since.
I have now been four months at a state of ZERO fatigue; and extremely close to zero with joint pain and stiffness. Unfortunately; I can’t say the same about the eczema skin condition. It was completely resolved for more than a month; but I’ve now gone back into a smallish flare up state ( I think this regression was due to overexposure to sunlight; and eating coconut oil too?). Still, my eczema condition is hugely better than before my vitamin A elimination diet.
Thinking Clarity:
Quite similar to the resolution of fatigue, and joint pain; my thinking clarity has vastly improved too. In the 2-3 months leading up to my eczema skin condition; I found my ability to think clearly, and to focus was very limited. It was like I had Attention Deficit Disorder at age 54. Charles Darwin described this as his “swimming head”. I find that a remarkably accurate description of what I was experiencing. I now have no trouble at all with staying focused, and I believe my thinking skills are completely back to normal too. This improvement happened at about week three of my vitamin A elimination diet. It was very significant, and very noticeable. I’d like to say I now have perfect thinking clarity; and no A.D.D. whatsoever.
I think it is important to point out that the improvements with fatigue, joint pain, and thinking clarity did not happen at all gradually. There was basically no noticeable improvement for the first 3-4 weeks. Then, almost abruptly, over a 3 day period, they completely resolved. So, that was a pretty amazing experience. It was also completely, and totally unexpected since my vitamin A elimination diet was attempting to resolve my skin rash. Call me daft; but I had no idea that all these conditions were related.
Making this connection; I believe that at least some kids with severe eczema are going to have an extremely difficult time in doing well in school. It is not just because they have itchy skin either.
Skin Nodules
I had hundreds of little skin nodules show up on my elbows, knuckles and a few on my face; at least a year before I had any real signs of eczema. These nodules disappeared around week three of my elimination diet. They are completely, and totally gone. They have never returned.
Depression:
You might assume that of course people with these diseases experience depression; who wouldn’t be depressed? Well; that is not the case at all. It is a toxin induced depression, or apathy. I never once felt sorry for myself; or genuine depression. After-all, let’s be real, this was just a rash to me. But, I did experience this weird sense of indifference (the first time in my life).
vision
Vastly improved; no longer blurry or dull. Isn’t that ironic. Vitamin A is critical for vision; and I remove it from my diet, and my vision gets better.
NIGHT SWEATS
For a year or more I was experiencing some significant sweating at nights; mostly around my neck and head. That is now completely; totally gone. Not a trace of it.
Inflamed and Thick Scaly Skin
And of course, these two diseases share the lovely symptoms of having holes burned in our tissues. Or regions of tissue that is turned red, inflamed, thick and scaly.
That has been a much harder one to completely resolve (at least for me). It is of course the big symptom that everyone focuses on. But, it is only one of the symptoms of these two diseases. As I stated above, I think it is very important to look at all of the symptoms together, then it becomes a much clearer match as to what is really causing these two diseases. Let’s look at this differently. IBD has its documented primary symptoms, and a bunch of others categorized as Extra Intestinal Manifestations (or symptoms outside of the gut).
What is being termed Extra Intestinal Manifestations implies that these symptoms are somehow being caused by the IBD, or are somehow complications of the disease. I don’t think that is the case at all. What if we move the primary IBD symptoms down to the same level as the other ones, and just consider them to all be symptoms of some other underlying root cause?
I think this is highly more likely. Now; what would happen if someone with one of these autoimmune diseases went on a vitamin A elimination diet? In my own personal case, it was diagnosed as severe eczema, and it now looks like this.
Let’s look at more connections with Vitamin A toxicity and Crohn’s
CRITICAL EVIDENCE: Accutane – a huge, and direct connection
“Accutane (isotretinoin) is a popular drug for severe acne created by Hoffmann-LaRoche Inc. The drug is linked to severe bowel disease and other side effects.”
“The medication is a derivative of vitamin A and works by controlling the oil in the sebaceous glands.”
“However, clear skin may be accompanied byserious side effects like Crohn’s disease.”
“Roche stopped manufacturing Accutane in 2009.”
Please read the source page for all the other horribleness this drug has caused, including birth defects. With this hugely important information; what have the medical community, and government agencies done to warn the general public about the dangers of too much vitamin A? Nothing; as far as I know.
This is bizarre to me since the official information from the National Institute of Health states thatVitamin A IS A DIRECT TOXIN at high doses. Here, we have drug companies marketing a product that is exactly that. What the heck did they expect to happen? Could this be worse? Well, here is an interesting bit of trivia about Accutane (isotretinoin). It was first developed as a chemotherapy drug, and is still used as one today. It is used for this purpose due to its ability to kill rapidly dividing cells. Maybe it is just me, but does it not seem to be a bit extreme to consider this an appropriate drug for reducing acne in healthy teenagers?
Accutane (isotretinoin) – is an ISOmere of Tretinion. Tretinion is all-trans-retinoic acid. This is a direct derivative of Vitamin A.
Therefore; it is quite well established by this situation that high doses of Vitamin A, in the form of retinoic acid, can, and has caused Crohn’s disease. That’s no surprise to me. But, the key thing to understand, is that Vitamin A is not a direct toxin just at high doses; that is a myth. It can be a toxin at any dose. Once again, it just depends upon what storage state your body is in when you have that dose. Therefore, it is relative. If you are in a saturated, or near saturated state; then any small, or even tiny dose is toxic!
So, what has happened with Accutane, and what can we learn from this? Firstly, what this drug has done is built up (saturated) the body’s store of Vitamin A. Secondly, this saturated state has very likely caused Crohn’s disease in multiple cases. This has been proven in courts. Thirdly, most of these people did not fully recover after getting off of the drug (but some did).
Why did they not recover? I think it is because they remained saturated with retinol and retinoic acid. What’s going to happen to it? Is it going to simply disappear? No, of course it is not.
It may also, and could very likely be that this high dose of retinoic acid had caused permanent liver damage. I don’t know; and have no idea really; I am just hopeful it is not the latter.
The authors are questioning this cause effect relationship. They conclude that it is not really conclusive, and that the very slightly higher ratio in people who had taken Accutane and developed Crohn’s as opposed to the general population is not very convincing. Statistically speaking, the evidence is pretty weak. Just based upon the raw numbers I would agree. However, there are quite a few documented cases where people started on the drug, developed Crohn’s, stopped the drug and then recovered. So, I think that is pretty strong evidence that there is indeed an association. Also, if we were to do face-to-face interviews with these people; that might give us a better insight. Not everything is reflected in the numbers. My guess is that these were mostly perfectly healthy people before they took the drug. I think after talking face-to-face with say victim number 5,000 we might not care about the numbers, or ratios at all.
Now, let’s dig into this causal association question a little bit deeper.
I think the authors of this report should have taken a bit of a different perspective on investigating this question. In doing so they may have come to a different conclusion. Firstly, the basic question they are asking is: “Did Accutane Cause IBD / Crohn’s”; and that leads them down a certain path of thinking. The key starting point in the analysis is the understanding that Accutane is Vitamin A (retinoic acid). Yes, the retinoic acid molecule is slightly tweaked. But, it is an isomer, having the same chemical formula, and the same functional groups. Reading about the genesis of this drug, the LaRoche people were looking to develop an anti-acne drug, and started with the knowledge that this drug would move into the sebaceous glands of the skin, and reduce the amount of the oil feeding the acne causing bacteria. This is a documented fact. Regardless, Accutane and Vitamin A (retinoic acid) molecules are nearly identical, and effectively function the same in the human body. I don’t think there can be much debate about this point. The drug did work as expected, and did dry the skin, and did reduce acne. It also caused birth defects just like high doses of Vitamin A have proven to cause. These are facts.
We all know that the body stores retinol (a food form of Vitamin A). But, the most amazing fact about the Accutane experience is that the body stores retinoic acid too. We need to remember this fact.
Okay, so now let’s ask the “Did Accutane Cause IBD / Crohn’s” question just a little bit differently. Since Accutane is Vitamin A (retinoic acid), we can ask: “Did Vitamin A Cause IBD / Crohn’s” ?
In order to investigate this question; we need to first research the accounts of people who have authentically chronically poisoned themselves with genuine Vitamin A ( nothing to do with Accutane, or even retinoic acid, for now).
There are lots (1000s) of people who have done this for various reasons (for some reason they thought it was good for them). There are many well documented accounts; and it is still happening today. See the many cases documented on the NIH pages and elsewhere. So, let’s just take a bit of a hypothetical example (use a real case if you want) of someone taking reasonably high doses of Vitamin A, daily, for say 3 years. Here’s the sequence of events:
@ 6 months ⇒ no adverse symptoms at all
@ 12 months ⇒ no adverse symptoms at all
@ 18 months ⇒ no adverse symptoms at all
@ 24 months ⇒ no adverse symptoms at all
@ 30 months ⇒ no adverse symptoms at all, hair getting oily
@ 36 months ⇒ no adverse symptoms, but maybe the skin getting drier
@ 36 months+10 days ⇒ huge adverse symptoms; skin peeling; lips swollen and cracked, hair falling out etc, etc, seeks immediate medical attention
This similar sequence of events is repeated in all cases of chronic Vitamin A poisoning. So, what is really happening here? The body is safely absorbing and storing all the daily doses until it gets to a slightly saturated point. It is important to understand that all those stored doses have not suddenly become toxic. They are safely stored. It is the additional doses that cannot be absorbed, or absorbed fast enough, that are now becoming toxic. What these people are doing is filling up their storage capacity for this substance.
Okay, let’s get back to Accutane. Remember these are mostly young people dealing with an acne issue. So, what is the sequence of events? It is going to be something like this (depending upon dose):
@ 1 month ⇒ acne gets worse ( documented as a side effect )
@ 6 months ⇒ no adverse symptoms at all, skin drier, acne clearing
@ 12 months ⇒ no adverse symptoms at all, skin drier, acne clearing more / clear
@ 18 months ⇒ stops doses, or reduces to only when required
At this point in time; the vast majority of them have not yet induced Crohn’s; or any other disease.
Firstly, let’s analyze this documented common side effect of acne first getting worse. It is actually not a side effect at all. It is perfectly logical, and should be expected as a normal progression of taking the drug. When they start on the drug, since it is in the retinoic acid form, the body is going to quickly start moving this into the sebaceous glands. In order to do that, it must first wrap that retinoic acid in a lipid. Then, in order to move this new toxic lipid into the sebaceous glands, some of the current non-toxic lipids are going to have to be expelled. This newly expelled (and non toxic) lipid now fuels and promotes the acne causing bacteria.
Next, and more importantly what these people have done is significantly elevated their body’s storage. Therefore, they have reduced their future storage capacity. These are generally young people, so they may have gone from hypothetically say 10% storage used to something like 30-60% storage used. What they have effectively done is removed say 2 or 3 decades of future storage capacity that would have been consumed by our normal North American diet. Once again, most of those Accutane molecules are not going to become toxic; they are safely stored by the liver.
Now let’s get back to this report questioning the causal association between Accutane and IBD / Crohn’s. What they are failing to consider is the time dimension. It is what is going to happen to these people in the future with regard to regular vitamin A consumption that needs to be considered. At some point they are going to reach an elevated storage level where newly consumed vitamin A molecules are going to become toxic. They are going to be toxic because the body has no place to store them. It is almost like a guy authentically poisoning himself with regular vitamin A; but it is just a bit worse actually.
There is a big time delay here; most likely in 2-5 decades for most people, between taking Accutane and getting disease. Therefore, rather than looking at a particular point in time (2010) to consider the ratio of people who took Accutane and developing Crohn’s they need to wait 2-3 more decades, and redo that ratio calculation. Just as importantly they need to expand the question to: “Did Accutane cause IBD / Crohn’s, Lupus, Eczema, Arthritis or any other autoimmune diseases?”.
There are more than 7,000 lawsuits filed over Accutane. I’ve read one report that it is projected that about 30% of the people who took Accutane will go on to develop Crohn’s / IBD. If that proves to be true, that will be more than 120,000 people. Now I think there should be little doubt about a causal association between Accutane and IBD.
At the very least we should be warning people who did take Accutane to start adopting a very low vitamin A diet. If anyone is wondering if I have a personal issue with Accutane; no I don’t. I did not take Accutane.
Therefore, the hugely important thing to learn from the Accutane disaster is that it is Vitamin A that caused the IBD / Crohn’s disease. Don’t just think “Accutane”; the product name, caused it.
Most importantly, we can now say: Vitamin A caused incidents of Autoimmune Disease. That should be a really interesting statement to stop and think about for a moment. Maybe for a very long moment.
Therefore, is it not highly likely that Vitamin A is still causing a lot more incidents of Autoimmune Disease? Could it be that it is causing most of these autoimmune diseases?
It does not matter at all if that vitamin A was obtained from an acne pill, or from eating fish, or tomatoes, or liver. In the end, it is all just vitamin A. It is a direct toxin! This is a simple scientific fact. The other simple scientific fact is that this direct toxin will cause inflammation and destroy human tissue.
Is there other supporting evidence in the geographic, and demographic, data with regards to Crohn’s disease? Of course there is. And like the Accutane disaster we have another man made disaster that adds significant evidence; the collapse of the Canadian East Coast cod fishery in 1992. More on this a bit later. Firstly, let’s deal with some of the common theories regarding these diseases.
What is NOT causing Crohn’s disease and Eczema
KEY EVIDENCE – It is not a modern environmental toxin
It is not herbicides or pesticides, or modern day pollutants, or chlorine in the water etc,. This is clear because these diseases have been around for over a 100 years. Darwin had eczema 200 years ago. Please see my post on that: New Lessons from Charles Darwin. This is not just out of some historical interest; I consider it to be more strong evidence supporting this theory.
KEY EVIDENCE – It is not genetics
The incidence rates of these diseases are doubling at alarming rates; like every 10 or 20 years. Human genetics are not changing this fast. Moreover, 20% of kids now get eczema, and most “grow out of it”. Likewise, teenagers and young adults “get” Crohn’s; and they did not have it during early childhood. That is just not logical if these were genetic diseases.
Kids would not “grow out of” eczema, and magically pick up Crohn’s at 15-20 years old. No way. You don’t grow out of a genetic disorder. And you don’t grow into one either; at least not on a wide scale; like what we are seeing with these diseases. If you really have a genetic disorder, you are most likely going to have it at birth, and you’ll have it for life.
What is probably a genetic predisposition is just the location the body is going to manifest this toxicity. Undoubtedly, some people have both Eczema and Crohn’s. I believe that if Eczema patients use steroid creams long enough; they are just going to force this inflammation to go internal.
The higher prevalence among Ashkenazi Jews is probably also not genetic. It is more likely simply due to their diet. Some customary dishes include chopped liver (53,000 IU/100g) and pickled herring (1,300 IU/100g). Other geographic distributions for these diseases is going to closely match dietary patterns. World incidence rates are going to closely relate to those areas with high cumulative consumption of vitamin A. Additionally, it is going to closely correlate with countries that fortify milk and dairy, and those regions with high consumption of cold salt water fish.
If these diseases were genetic; then the severe symptoms would probably be much more consistent. There would not be this sporadic-chronic nature to these diseases. We would not see these periods of remissions and “flare-ups”. The genes are not going into remission, and recurrence. What is causing the “flare-ups” is far more simple; it is food. And no one stops eating vitamin A! It is nearly impossible; it is everywhere. What is sporadic; is just the amount of intake; and the current relative level of saturation. If these diseases were genetic disorders, they would not go into remission for months, and years.
Oddly, everyone in the eczema community agrees on the foods that cause the “flare-ups”. This includes the American and Canadian Eczema Associations. The cited trigger foods are like: eggs, milk, dairy, fish, tomatoes, red peppers, and citrus fruits. This is documented over an over. It is similarly documented for Crohn’s and Lupus, and other autoimmune diseases; just not so specifically. But, the key point is that we have a list of foods that “trigger” “autoimmune” disease flare-ups. But, are not “trigger” and “auto” kind of contradictory terms? Why aren’t people considering that these are not just the “trigger” foods? Rather, are they not the actual root cause foods too?
All I did was to ask myself a simple question: what do these “trigger foods” all have in common? The “trigger foods” all share a common fact. They all have high levels of vitamin A.
Now, if you are not familiar with adult eczema; you would very reasonably conclude that; no problem, just stay away from the documented trigger foods and you’ll recover.
Well, this is the apparent paradox in this disease. The trigger foods can definitely make it worse; causing flare-ups. But stopping these trigger foods does not cure it for most people ( it has for some people). It just brings it down to kind of a baseline.
People don’t cure from it because they are in a saturated, or near saturated state. They can mostly avoid the big flare-ups. But, just the regular daily intake of vitamin A is enough to keep them in the perpetual state of subclinical toxicity. To even begin to recover; they need to adopt a zero vitamin A diet. This is almost impossible to randomly ever happen. Based upon my experience, once you do adopt a zero vitamin A diet; it takes at least a week to start to see results, and 5-6 weeks to see really big results. Foods that are labeled as 0% RDA are only really low in vitamin A. That is almost meaningless. I think you need foods with 0 molecules of vitamin A.
KEY EVIDENCE: It is not truly Autoimmune
This one is not so obvious. The immune system is definitely involved here. But, not in the defective way that it is believed and documented to be. The immune system is not randomly attacking the cells at all. It might just appear to be what is happening. No; the immune system is working just fine, and trying to deal with a toxin; or a toxic situation. I don’t know the exact mechanism; but I do present some plausible explanations.
There are some really big clues here with the steroid creams used to treat eczema. For argument sake, let’s say the immune system is attacking the skin tissue (the assumption being that these are defective, or out of control, rogue immune cells). I am calling these rogue cells because the inflammation is not body wide; but quite localized.
Now we apply the steroid cream (immunosuppression) to the location of the inflammation. It works like a charm (firsthand experience). The immune cells back off, and the inflammation dies down quickly. Did we kill these rogue immune cells? No; we did not. What happens to them? Do they move on and immediately attack tissue elsewhere? No, they do not. Therefore, what we’ve really done is to introduce a immunosuppression agent to the site of the inflammation. These rogue white blood cells, and every other white blood cell in the body is now staying away from this location. What we’ve really done is to put an immune barrier around the site of a substance the immune system regards as a toxin. Technically speaking; we are blocking the production of cytokines that call the immune system into action. Therefore, logically, these rogue white blood cells are not rogue at all. The are normal. They are just getting the wrong messages.
Therefore, I think it is far more likely that the retinoic acid (or some other form of retinol) is building up in the tissue, and dissolving collagen, and this chemical is destroying cells. These tissue cells are under attack from this toxin and they are sending out some signal to the immune system for help. The immune cells are rushing in to the fight; but they are not equipped for this battle. The body has just not evolved for this. This is the liver’s job to protect the body from this potential toxin. But, the liver is maxed out; it is now sidelined, and of no help. Thus, free retinol is relentlessly entering the bloodstream with every meal. We are now in subclinical toxicity; it only appears to be an immune disease that is causing the destruction.
If the immune system leaves this potential toxin circulating in the blood, it will burn holes in the kidneys, brain, and other organs.
There are even more reasons that this is not “auto” immune. Why are these very localized inflammations we see in these diseases? I am not talking about all autoimmune diseases combined. I am talking about just in the context of one of them; such as eczema, or Crohn’s, or pick almost any other one of them. Even arthritis; it does not attack every joint in the body; only some of them. Eczema does not attack all the skin; only small parts of it. Therefore, the immune system does not have an issue with these tissue types. Rather, it has an issue with these tissue types at only specific locations.
If the immune system had gone haywire; it would be far more widespread; if not everywhere. In the case of eczema; almost all of the skin should be under attack; and not just these limited little patches of it. That is just not logical.
Likewise, it is just not logical that the immune system would magically stop “auto-immuning” and start up again, in some random fashion that we see in these diseases.
Why does the immune system stop “flaring-up” and the disease go into remission? Does the immune system get tired of the fight, and give up for a while? Does it need time to rebuild resources before the next attack? Isn’t it far more logical that it has actually accomplished what was needed, and finished its job?
What is random is the amount of vitamin A we eat, and the relative states of the digestion and absorption rates our body can sustain. Amazingly, there is another tricky factor at play with eczema, and that is the weather. Eczema, Lupus, and Arthritis sufferers commonly report that these conditions get worse in the winter. Here is an interesting study referencing this point on winter conditions affecting an autoimmune disease.
Efficacy of dietary hempseed oil in patients with atopic dermatitis (Eczema). http://www.ncbi.nlm.nih.gov/pubmed/16019622 Department of Pharmaceutical Chemistry, University of Kuopio, Finland.
This is important because skin dryness and subsequent itchiness often lead to the use of medication in atopic patients, especially during the dry winter conditions in Finland, where ambient indoor humidity can be <30% moisture for months on end.
What the heck does the weather have to do with an autoimmune disease? That should sound absurd, but it is not. It is perfectly logical. It’s not the temperature, or the air pressure at play here. It is the moisture level dropping, and, to maybe a lesser extent, the reduction in UV exposure. We’ll come back to this topic a bit later.
For what it is worth; I believe I am able to turn off and turn on my auto-immuning, as if by turning a switch off and on. Only, the switch is food with and without Vitamin A. I am able to do this because I’ve been on a near zero vitamin A diet for months now. Naturally, I am trying, very, very hard to keep it turned off. It is a struggle; it is tricky, and I am still dealing with it every day. There is still a huge amount of retinol, and or carotenoids stored in my body.
KEY EVIDENCE: Skin Fluorescence
To investigate this point I compared my brother (two years younger), and myself under a fluoroscope (a form of a black light). It is an old geology fluoroscope that I have, and I am not sure of the exact wavelength. Nevertheless, it worked great. It induced a huge amount of fluorescence in my skin; but not in my brother’s.
Wow! it was a shocking difference. I clearly have a large amount of carotenoids and /or retinol in my skin compared to him. Why is that? Well, consider what my brother’s diet looks like, Coffee and toast at breakfast; burgers at lunch, and steak and potatoes for dinner. He drinks beer, does not smoke, and does not drink milk. He is perfectly healthy. No sign whatsoever of inflammation, or skin diseases, or any other disease. How’s that for ironic? I’m the one that eats “healthy” and I get diseases; he doesn’t, and he’s just fine.
I’ll try to post some pictures of my face under florescence. However, my current camera does not pick up the emission wavelength very well. But, I do have a few pictures of my hand and skin florescence in my photo gallery.
Therefore, this fluoroscope test would be a simple, simple, noninvasive technique to quickly evaluate the levels of carotenoids and /or retinol in people. Note that retinoic acid is not florescent.
The wavelength used might need to be adjusted to pick out each compound (carotenoids and /or retinol). Nevertheless, it is more direct evidence. You can literally see it glow under / in the skin. If anyone is doubting this; well just check for yourself, and post a comment as to your observations.
KEY EVIDENCE: Randomness and symmetry
In addition to the intense immune response not being body wide; an even more important observation to make is that it is not in completely random locations either. For most people, eczema is much more common on the hands and face and the back of the scalp (in children).
What is common about the hands and face? Both are exposed to sunlight. Both retinol and carotenoids are light sensitive molecules. Sensitivity to sunlight is a well documented symptom of vitamin A toxicity, and of course of Lupus too.
However, eczema does indeed commonly show up in locations where there is no exposure to sunlight; such as the underarms, the elbows, behind the knees, and even the tops of the feet too. So, it is not just sunlight that is invoking the immune response. It is a toxin. How about a toxin that is also a light sensitive molecule?
Not only is it not completely random locations that eczema shows up at, it exhibits some symmetry on the hands. For me, this is the ring finger of both hands, and the space between the thumb and the index finger. Placing both hands face down on the table, index fingers and thumbs touching; the inflammation locations are actually symmetrical. These are not quite mirror images; but close enough to be very significant.
Now, how can the immune system mount a coordinated and symmetrical attack like this? That is just not at all logical for even a healthy immune system; never mind a defective one. No way is this the immune system choosing these locations to autoimmune at and attack my skin cells. It is far more logical that there is something common about the locations that makes the immune system want to attack here. I know it sounds like semantics; but there is of course a big and very critically important difference in who is initiating the immune response. Meaning; did the immune system itself; or did skin cells call the immune system into action. Since these are symmetrical locations; I think it should be clear that the immune system is responding to something at these locations; it is not the immune system randomly autoimmuning.
I have an old family medical textbook, that was published in 1964. It has a good chapter on Eczema. It documents that the most common place for eczema to first show up is on the ring finger. Exactly the same goes for me now; 50 years after that publication. So, with the immune cells circulating in the blood; why do they prefer these locations to autoimmune at? We have this well documented, and common location for autoimmuning to take place. Isn’t that kind of amazing for a defective immune system to be this consistent?
Therefore, I think it is obvious it is not a defective immune system at all. Clearly, there is something at these locations that is invoking the immune response.
An analogy would be to notice that the police are commonly showing up at the houses of drug dealers; and causing altercations. Then, observing and being alarmed by these altercations, concluding that the police are defectively auto-policing, and are wrongly attacking the same citizens houses all the time. No; there is a reason the police are going to these same locations, just as there is a reason the immune system is attacking the skin at these preferred locations. It’s their job.
White Flaky Skin
A documented secondary symptom for eczema is white flaky skin. I’ve closely looked at the skin at the sites of inflammation under a 30x microscope. I have always seen white flaky skin on the top layer. This top layer of white flaky skin is always present both with the inflammation, but more so after the inflammation dies down. It might be a bit hard to see when the skin is highly inflamed, and turned red. But, if you look with a 10x-30x microscope you will see it clearly. Here’s a picture from wikipedia.
Please ignore the red, inflamed skin in this picture for now; just take notice of the significant white skin flaking off. Of course, white flaky skin is not only a well documented symptom of vitamin A toxicity; it is actually one of the key symptoms. So, the important question is how does the immune system cause this? Does it burn off the very top layer of skin? What’s really going on here? I think it is the overgrowth of the skin being induced by a growth hormone. This is exactly what is documented to happen in the presence of retinoic acid.
KEY EVIDENCE: Hair Burnt Off
There is another key observation to be made while examining the skin under a microscope (repeatable by anyone with severe eczema using a magnifying glass). The hair on the inflamed skin is often burned right off too; almost like it has been shaved off with a razor. This is not just a few hairs burnt off; it is 100s of them; all at the same depth. The exact location (depth) of this burn off on the hair is another very important clue. It is just a bit deeper than the top surface of the skin; maybe 0.5 mm below it. But, it is actually not burned out into the root of the hair follicle.
It is burned off right above the sebaceous gland. The deeper hair follicle is intact.
Now, why would the immune system burn off the hair shaft right at this level, and not burn it off, or deeper, below the sebaceous glands? It is much more logical that whatever is coming out of the sebaceous glands has burned off the hair at this level. I think this depth that the hair shaft is being burnt off at is a very important clue; and we should not gloss over this. What exact chemical is capable of burning off the hair like this? What is the concentration of retinoic acid within these hair follicles?
It is interesting that Accutane is documented to work by controlling the oil in the sebaceous glands. Accutane is retinoic acid. It does not really control the amount of oil in the sebaceous glands; rather it toxifies it. The retinoic acid builds up in the lipids in the sebaceous glands. Yes, this is documented, and well known; and Accutane clearly proves this. It has been proven like 400,000 times over. Now, with the retinoic acid within the lipids contained in the sebaceous glands; and at elevated levels, the sebaceous glands can no longer moisturize the skin. They do the exact opposite; they dry it out. It is a vicious cycle actually. As the skin gets drier; even more oil is released from the sebaceous glands; as that oil is consumed, even more retinoic acid is exposed, and the skin gets even drier. We now get inflammation; and if it is severe enough; eczema.
This is going to cycle until the sebaceous glands get temporarily depleted of their fat store. We are now in a “flare-up” mode. Of course we now have a direct toxin within the skin layer. The immune cells are going to respond, and try to contain and remove this toxin. Where to? Maybe back into the sebaceous glands?
This also completely fits with the widely accepted view that eczema, psoriasis, and lupus all get worse in the winter. And this is why you need to moisturize yourself within 3 minutes after the shower.
This also correlates with my other observations that more often than not there is slightly more inflammation right around the hair follicle as compared to the surrounding skin. Secondarily, when the little burn craters show up, they are somewhat more prevalent just adjacent to the hair follicle too; usually say 1-3 mm away. But, the little burn craters are not at all exclusive to being adjacent to the hair follicle; they are indeed wide spread throughout the inflamed skin area.
There is another interesting observation in that 1964 family medical textbook of mine regarding eczema. They report that eczema on the hands is much more common in women who washed dishes; and recommended using gloves. Okay; after reading that sentence; does anyone seriously believe this is an autoimmune disease? How can the immune system know that someone is washing dishes; compared to some other activity such as typing, or playing the piano, or anything else? That is just so completely nonsensical. Of course what is happening is the dish washing is drying out the hands; and that has the same effect as the dry winter air. That causes sebaceous glands to release stored fat / oil with its contained retinoic acid. As the skin absorbs and uses that fat; it exposes the retinoic acid molecules. And clearly, eczema is much more than just dry skin. Let’s not get confused about that. Eczema is inflamed, burning, peeling, cratered, weeping skin. We have a vitamin A acid peel right inside the skin!
Lastly, I think we can more or less prove that Eczema is not “auto” immune with a trivial little experiment. Anyone with severe eczema can repeat this same experiment in just one minute.
Steps:
Find a location that has some very slight swelling to it; but has no redness whatsoever. (For me I’ve commonly had this condition on the backs of my fingers just above the metacarpal bone.)
Firmly (but not too hard) rub that area for 30 seconds; don’t scratch at all.
What happens? Within a minute, or less, that area will start to become inflamed; and red with the start of the eczema condition. I’ve now induced the autoimmune response at exactly this location. Yes, no question the eczema condition was going to happen in a few days anyway; I’ve just significantly sped up the process. How long does the red inflammation at this location persist for? About 4 to 6 weeks! (weeks is not a typo). It finally heals when the very top layer of white flaky skin forms, and flakes off.
Repeat this same experiment at another location where there is no prior swelling. For me; I’ve used my thigh. I can rub it for five minutes; no redness; no autoimmune response; no eczema. Rubbing the skin here does not cause an immune response.
So, the obvious question is: how can just firmly rubbing the skin for 30 seconds invoke an autoimmune response that lasts for over 4 weeks? It is just not logical that this action alone caused my white blood cells to attack the skin at this location; and to continue doing so for the next 4 to 6 weeks.
What is far more logical; is that this rubbing has put pressure on the sebaceous glands, or other fatty structures, and squeezed some of the contents to go in between the layers of the skin. I’ve just forced some toxin to be exposed. The immune system is responding to that toxin; or more correctly the immune system is reacting to the effect the toxin is having on the skin cells themselves.
Why does it take 4 to 6 weeks, or longer to heal? I have no idea. A few weeks ago, I scratched the back of my thumb on a nail; it was quite a deep scratch; with some bleeding. That scratch took 7 days to completely heal. So, I think the healing time for my skin, and my age, is about 1 week. Why does this eczema take so long to heal? It must be that this toxin is really hard for the immune system to deal with. Maybe it takes 4 weeks for the immune system to gather this up, and put it back into the sebaceous glands? More likely we are kicking off a nearly endless chain reaction.
critical EVIDENCE: The Koebner phenomenon
Once again, this is not just my observation. It is well documented; and of course has its own name. It is called the Koebner phenomenon. It is reported particularly within patients with psoriasis and to a somewhat lesser extent with eczema. It also occurs more often in the winter, than in the summer. The cause of Koebner phenomenon is documented to be unknown. Well, I don’t think it’s a phenomenon at all. I think it is a little yellow toxic molecule embedded in lipids in the skin layer, and in the sebaceous glands, that is being exposed when the skin is being pressured. And this is why Eczema is indeed the scratch that itches. The more you scratch, or rub, the more toxin you expose.
More thoughts on The Koebner phenomenon
When I first read about the Koebner phenomenon it was a bit surprise that this goes back well over 100 years ago and that it has not been solved. I think if the Koebner phenomenon were to be solved, the entire enigma of autoimmune diseases would be quickly unraveled.
To me, I think it is obvious now. There is a toxin already in the skin; and it has been sitting there for a long while. That toxin is now being exposed; or released as a result of the pressure on the skin.
For the medical researcher; that might sound absurd. They might logically ask why would there be a toxin stored directly within the skin? That’s nuts! But, it is not. It is completely logical. To a layman like myself; it is more like “what else could it be?”.
It is very interesting that the Koebner Phenomenon is documented to occur in people with psoriasis, eczema, systemic juvenile rheumatoid arthritis, vitiligo, lichen planus, et al. It is also documented to be All or Nothing like. Meaning that you can reproduce it in only people who have these skin disorders; but it is never reproducible in people who clearly don’t have these diseases. Since the Koebner Phenomenon is unique to people with these diseases; I think it is hugely likely that if we can determine its true underlying mechanism; then we can quickly get to the root cause of the disease itself. It is not at all surprising to me that juvenile rheumatoid arthritis is on this list either.
I’ve personally reproduced the Koebner Phenomenon on myself multiple times, and have caused my eczema to spread. I am able to spread out my autoimmune disease area as if it were an infection. Of course, I am not spreading an infection. I am spreading a toxin with its corresponding complicated chain reaction.
The facts we know with certainty are:
We know from Accutane that the body is going to move retinoic acid laden lipids into the sebaceous glands in the skin.
We know from the Japanese and Brazilian researchers that retinoic acid applied to the skin does cause the Eczema rash, and rapid skin cell growth.
We know from the global observations that eczema and psoriasis worsen, or flare-up, in dry weather. This is clearly happening when the skin is absorbing the oils from the sebaceous glands.
Therefore, I think the Koebner Phenomenon offers a huge and immediate opportunity to reveal the root cause of these diseases. It is a toxin sitting within the lipids in the sebaceous glands. We know the exact toxin we are looking for too; it is retinol, and / or retinoic acid. I suspect the retinol mostly; due to its fluorescence.
There is absolutely, 100% positively, something in my skin, and it is fluorescent. It is not slightly fluorescent either. It is hugely, and shockingly fluorescent. There is not a wide range of possibilities as to what this fluorescent substance is. You don’t need biopsies, or sophisticated equipment to see it either. I am seeing this with a $300 fluoroscope. Once again, retinoic acid is not florescent; so I may be seeing only a portion of the amount of the retinoids stored in my skin.
Since retinol and retinoic acid are a very light sensitive molecules; anyone wanting to test this theory needs to be very careful in obtaining and testing a sample. But, I think this could be proven in a matter of days.
Eczema is clearly not random autoimmune activity. It is due to a toxin found in the sebaceous glands, and elsewhere in the skin lipids. Maybe the high levels of vitamin A actually burn out and destroy the sebaceous glands too. I don’t know.
What does this mean for Crohn’s? Well, I highly suspect that we are going to see almost the same appearance in the tissue being surgically removed from people’s GI tract, and / or in anal fissures, etc.. What about inspecting this tissue under a fluoroscope too?
The question I was really curious about was: does the tissue in the GI tract also have sebaceous glands or similar lipid containing structures? Yes, it does. Not only that, the intestinal tissues store abundant amounts of vitamin A. Why is it here? It is used by the dentritic cells. The dentritic cells are part of the immune system. Dentritic cells in the lining of the intestine are always busy swimming around locating, engulfing and destroying the many pathogens that end up there. While doing this, they convert some of the retinol (vitamin A) stored there into retinoic acid. Could it be that the dentritic cells use the retinoic acid as a form of chemical warfare against pathogens? This fits with the observation that infectious diseases depress circulating retinol and contribute to vitamin A depletion.
Additionally, these dentritic cells have some very cool little features and capabilities. They have tentacle like protrusions that penetrate the tight junctions between the epithelial cells, through to the other side, and use these tentacles to take external surface antigens back in for destruction. Just to clarify this; this is internal immune cells reaching to the outside environment to grab antigens. How cool is that? Moreover, and very importantly I think this might explain the intense itching people with eczema experience. It sure fits with the weird tingling feeling I often had on my face.
The insides of the cheeks have sebaceous glands too. So, I think I now know why I was getting the canker sores too.
Okay, let’s get back on track here. So why would anyone think that Accutane, or elevated levels of retinoic acid in general, is not going to dry out, and cause inflammation in this tissue too or anywhere else in the human body?
What is the real cause of these diseases is the relentless, and subclinical poisoning from vitamin A in our food. But, it is a subclinical poisoning only if you’ve reached a near saturation storage level.
Do you think this is too bizarre to be true? It is not. It is just assumed to be impossible, and not happening on a wide scale. Guess what? Charles Darwin got himself into exactly this state too, and remained there for his entire adult life. This was a missed lesson for us.
Is it a coincidence that some of the most common places for Lupus rashes, and eczema, and psoriasis to show up is on body locations that have the highest concentrations of sebaceous glands; such as the face an scalp? We now have lots of kids 2 & 3 years old that still have “cradle cap”. Oh, and now the same goes for lots of guys 50+ years old too.
After the Accutane disaster it should have been abundantly clear that people could get too much vitamin A, and directly cause serious, deadly diseases. This was another missed lesson for us.
Were there any general warnings issued to the public? Were cod liver oil, and vitamin A supplements pulled from the stores? Does liver at the meat counter have a toxic chemical warning sticker put on it? No; nothing as far as I know. Maybe just the opposite happened; via more regulation to supplement more foods with this potential toxin, and mandate the use of carotenoid based food coloring everywhere.
A more in-depth understanding of Eczema
There are like 20+ million people with this disease in North America. It varies from very mild to very severe, it varies from random occasional occurrences, to horrible unrelenting flare ups. It varies from the very young to the very old. Infants get it, and people 80 years old get it for the first time.
People with eczema more or less all know that it is food related. The eczema medical community recognizes this too. But it has just not been recognized yet as being a form of vitamin A toxicity that is the real cause. Nevertheless, since it is so visible, and people can more or less see responses due to diet changes, there is an opportunity here. But, like all of this; it is tricky. There are some big buffers between consumption and resulting skin changes. If you stop consuming vitamin A there maybe very little immediate improvement in the skin, or even for a very long time. This is because the skin has its own reservoir of internal storage. Additionally, you can still experience a flare-up many months after adopting a low vitamin A diet. This is because you may not expose the embedded toxin until your skin is exposed to dry winter air, or some other drying condition.
Sadly, like Crohn’s disease; researchers have been looking for the cause and cure for eczema for well over fifty years, maybe even 200 years. As far as I can tell; no progress has been made at all; like zero.
Who “gets” Eczema?
Generally, there are two big age groups with Eczema. Young children, and adults starting around age 50. Most young children grow out of it. Some don’t, and have it all their lives. When adults get it, it is more or less chronic; comes and goes, but almost always comes back. It usually worsens as we get older. Why is that?
When someone “gets” Eczema; what exactly do they get? It is not a bacteria, it is not a virus, it is not a fungus. Did they get a genetic mutation, like in Cancer? Not that either. It is a randomly defective immune system. An immune system that is randomly attacking the body itself. But, hold on, isn’t it the primary job of the immune system to protect the body? That just seems so peculiar to me. But, hey, I am open minded; anything is possible. But why do 20 million people in North America “get” eczema; and there is no where near this rate in India, or China, or Russia?
My theory is that young children are simply surging their vitamin A intake past their maximum absorption rate. Their available absorption rate is simply proportional to the size of their liver. The volume of the liver is increasing at a rate about exponent 2 of its cross sectional size. The absorption rate (the rate it can absorb and safely store vitamin A is going to be directly proportional to the remaining storage capacity) is generally going to decline with age; especially if you live in North America, due to accumulative consumption.
Why is this Age incidence pattern occurring in Eczema?
If children eat a reasonable diet, the growth rate of the liver, and its absorption rate will exceed their dietary intake. The absorption rate curve and digestion rate curve will diverge, and they will move out of the toxic state. If, on the other hand, kids eat lots of milk, dairy, pizza, tomatoes, fish, brightly colored fruits and vegetables; or horror of horrors, take cod liver oil, or eat liver, they are doomed to stay in this toxic zone for the rest of time. The absorption rate curve and digestion rate curve will converge. Oddly, even candy may be a contributor, since it is colored with carotenoid based food colors.
On the other end of the age spectrum, we have people my age; 50ish. We did not grow up in this insane childhood food environment we now have. So, we escaped childhood without Eczema, or Crohn’s. However, we’ve made (at least I have) the big mistake of listening to the current nutritional advice; taken fish oil, frequently ate fish, and lots of milk and dairy, and brightly colored fruits and vegetables too. Our healthy eating has caught up with us. We have slowly built up to the same saturated state. Unfortunately, unlike children, our liver is never going to grow larger to save us. It very well, and probably is, all swollen up, and fatty doing everything it can to try to save us. It may actually start to shrink in physical size as we age too. I don’t know. Whatever the mechanisms, we have this big U shaped curve with incidence rates; lots of kids, and a new up trend around age 50. This same U shape type curve applies to the incidence rates of other autoimmune diseases too.
Since vitamin A is a fat soluble molecule, the liver must then store it in a fatty chemical safety blanket. So, of course a fatty liver is now the norm for people over 50. Sadly, in Canada it is reported that a significant percentage of kids could have fatty livers. It is a somewhat of a hidden epidemic.
Let’s consider this in the most basic way possible. The liver stores vitamin A, but it first must be wrapped it in a fat to safely facilitate that storage. With the consumption of vitamin A vastly out of control in North America, how could we possibly expect people to nothave a fatty liver? Isn’t the body doing exactly what we should expect it to? What am I missing here?
Okay, so now at 50+, we are in big trouble with Eczema. The same applies to the 50+ folks getting Crohn’s and other autoimmune diseases. Now, let’s get back to the other end of the age spectrum.
KEY EVIDENCE: Crohn’s incidence rates kicking in at age 20ish
The really interesting question here is: what is this magic 20ish age thing with young people getting Crohn’s. What happens at that age in the human body? Take just one guess, you’ll probably be right.
The human liver becomes fully developed at age 20ish, boys are 1 or 2 years earlier. So, that is probably why there is this spike in Crohn’s at this age. The growth of the liver can no longer outpace the rate of dietary consumption of vitamin A. The race is lost. Of course, it is not this binary. This can, and clearly does happen at any age, between 10 and 50+. That 20ish age also corresponds to the post acne age too. How many of these young people took retinol based acne medications?
I have no doubt that kids younger than 10 surge their dietary intake of vitamin A, and cause a burn in their bowels. Unlike 10 year old kids with Eczema, they just can’t see it happen. They may just get an unexplainable abdominal pain that lasts for a few days, or more. The damage is painful, but silent and out of sight, The body heals, and they move on.
KEY EVIDENCE: The higher socioeconomic status factor
People with higher socioeconomic status have a higher prevalence. We need to ask the all important: why is that? question. I can guarantee that the immune cells cannot detect their bank account balance. But, there is a reason. It is because they are likely to be more educated, and have more money to spend on eating healthy with lots of brightly colored fruits and vegetables, and maybe vitamin supplements too. There is the same higher socioeconomic connection with rates of Crohn’s, and Alzheimer’s too (in the USA). Is this true of Lupus too?
For me; this higher socioeconomic status connection is a super important key point.
It is not just an interesting anecdotal finding. What does this key point really tell us? It tells us; in perfect, indisputable clarity that these are not genetic diseases. They are also not environmental, in the terms of the air we all breathe; or the water we all drink, or exposure to farm toxins etc. They are also not from some gut bacteria, or lack thereof. What is different is the food people choose, and what they can afford to buy. It is the FOOD!
What food(s) exactly? Once we can answer that, then we need to ask an even more important and specific question. What exact chemical compound(s) in those foods is it?
KEY EVIDENCE: Nova Scotia, Canada
About 10 years ago, I listened to a news report about Halifax Nova Scotia having the unfortunate distinction of being the Alzheimer’s capital of Canada (in rates of incidence). I don’t remember the exact numbers, but it was something like 1.5x or even 2x the national rate.
Researchers were trying to understand why. Well, I think I now know. As I’ve stated above, I think Crohn’s, Eczema, Arthritis, probably Lupus, and Alzheimer’s all share the same sinister parent.
When I first started looking into Crohn’s; it was only a bit surprising to find out that Nova Scotia also has the highest rates of Crohn’s and Colitis disease in the world.
So why is it that both Crohn’s and Alzheimer’s rates are really high in this province? Well, it should by now be obvious to us. It is that this province has been historically very high in fish consumption. It was actually a fish based economy, and a of course a staple in the diet, from like the beginning of time. But, the key, key point here is that it is not just any fish. This is Atlantic Fish.
Remembering the news story about Alzheimer’s being high in Halifax, and believing there is a connection between Eczema and Alzheimer’s, I told my wife that I’d expect that there would now start to be a significant drop in incidence rates in the province. Why?
It is because in 1992 the fish stock collapsed under the burden of overfishing by the industry. The government imposed a fishing moratorium, and all commercial cod fishing was stopped.
it was observed that there has been a significant decline in the incidence rates of Crohn’s in the province starting around 1996, and continuing through to now. It is like a 25 to 35% drop. This is a really significant finding. The diet in Nova Scotia pre fishing collapse of course very much included cod. That changed almost abruptly, starting in 1993. A very important observation to make about this report is that the age group with the biggest decline in rates is the 20 to 29 age group. Since the Atlantic cod fishery had been closed for nearly their entire lives; this makes sense.
I was really curious what is happening with the incidence rates of Alzheimer’s since then.
Nevertheless, let’s get back on track here with Crohn’s and Eczema. What’s Atlantic cod fish high in? Surprisingly, Atlantic cod is significantly higher (10 x) in vitamin A than the same species on the Pacific West Coast.
Even though the meat of the Atlantic fish is 10 times higher; overall, it is not particularly high in itself. Once again, we need to factor in the TIME dimension here. One cod fish meal is not going to do any harm. But, 3,000 or more of them will. Additionally, the cod oil is much, much higher in vitamin A.
There is no doubt that the decline in incidence rates of Crohn’s in the province is due to the abrupt reduction of Atlantic cod fish in the diet. So, in one man-made disaster (Accutane), we added vitamin A to people, and caused more Crohn’s. In the other, we removed a significant source of vitamin A from the diet, and subsequently hugely reduced the rates of Crohn’s. These are not coincidences. These are facts that cannot be ignored.
On one hand, we have just (inadvertently) conducted a ~20 year, ~5 million person field trial with the closure of the Atlantic Cod Fishery. This has led to a very significant result, specifically with regards to Crohn’s. But, on the other hand; there could be something wrong in my determination that cod (the meat) is the culprit here. Cod meat is actually not that high in vitamin A ~ 100 IU / fillet. However, a kid growing up in Halifax eating cod three times a week, compared to a kid in Alberta or Saskatchewan eating beef three times a week, will consume about 500,000 to 1,000,000 UI more of vitamin A over a 20 year period. These may look like big numbers; but they are not really in the context of Vitamin A consumption. Therefore, this should be a very clear indication that the truly safe range of consumption of Vitamin A is not very wide.
Now, as everyone knows; the cod oil is much higher in vitamin A. So, we need to know what happened to the oil (especially the liver oil) from these fish?
Did this go into the food chain somehow. Was it used for cooking; or supplements etc.? Basically, was it consumed by people in this Atlantic region, and the US Atlantic coast too? I am guessing; probably yes. But I don’t know the pathway. Please comment if you can. Also, please comment if you can on the rates of other diseases in the region over this same time frame. I know that Atlantic Canada has historically been somewhat higher in rates than compared to the rest of Canada. What about rates in Sydney Nova Scotia over this time frame? Sydney had some of the highest disease rates in Canada in the 1980s and 1990s. In a news report from the Halifax Herald in 1998, they state: “Deaths caused by hypertension, Alzheimer’s disease or multiple sclerosis occurred at twice the national average in Sydney.” The report cites the Sydney tar ponds as the suspected toxic source. But, I wonder, has that now changed too?
The Crohn’s & Colitis Foundation of America report in their 2014 Fact Book that the countries with the highest rates of Crohns, and ulcerative colitis are Canada, Denmark, Iceland, and the United States. But, more precisely this list should be: Atlantic Canada, Denmark, Iceland, and the United States. What is common at least between Atlantic Canada, Denmark, Iceland? It is North Atlantic fish consumption.
I think the USA is supplementing more foods with Vitamin A than does Canada. I’ve noticed that some simple foods; such as those with flour list vitamin A in the nutrition label; whereas the same foods in Canada do not. For example, plain Cheerios in the USA list 10% RDA without milk and 15% with milk. Whereas the apparently same box of Cheerios in Canada list 0% RDA without milk, and 6% with milk.
There is more evidence that can be gleaned from the closure of the Atlantic Cod Fishery event. It was not only Canada’s fishing fleets off the east coast; other nations had fishing fleets here too. When the cod fish stock collapsed, then these other nations stopped fishing here too. Therefore, we might see a decline, or maybe just a leveling off, in the incidence rates of Crohn’s in their home nations. Please help with more data if you can; see Collapse of the Atlantic northwest cod fishery.
But; just like with Accutane the drug name, we can’t implicate Fish, the animal name in these diseases. It is a chemical that is both in the Accutane and the Fish that is the culprit here.
For example, if we try to correlate incidence rates between say families in both Halifax and Victoria BC, that eat cod fish three times a week, that won’t work. But if we consider that the family in Halifax may actually be consuming 10x the vitamin A of the family in Victoria; we might pick up the connection. The same goes for other countries, such as Sweden and Finland that eat a lot of cold salt water fish.
“Novel findings include the demonstration of higher eczema prevalence along the East Coast. The study correlates well with previous reports and may help point to environmental factors that contribute to the development of eczema.”
Why? Once again, it is due to the higher east coast fish consumption. East coast cod fish is particularly high in vitamin A.
Other countries with high rates of fish consumption also have high rates of Eczema and Alzheimer’s, and I have no doubt Crohn’s and Colitis too. Here’s a world map showing Vitamin A deficiency. http://en.wikipedia.org/wiki/Vitamin_A_deficiency
Since it is a Vitamin A deficiency map, you just have to note that the dark green countries areas are getting at least enough Vitamin A. There are no surprises there for North America, the UK, Sweden, and Australia. But look at Chile. Chile now has the highest per capita consumption of fish in South America. It also has the highest rates of Alzheimer’s in South America. What are the rates of Crohn’s in Chile? What fish species do they eat? What about their tomato consumption too?
Here is another excellent study showing a global map of Crohn’s disease.
The comments regarding Chile are: Cases of 1996-2002 more than double compared to 1990-1995. Wow! More than doubled in just 5 years! What in their diet has changed? By chance, did they buy the unused Canadian fishing ships?
In the comments section of this report the authors ask:
“What unites Canterbury in New Zealand, Nova Scotia and Manitoba in Canada, Amiens in France, Maastricht in the Netherlands, Stockholm in Sweden, and Minnesota in the US (apart from the existence of scientists alert enough to reveal the evolving epidemiologic trends)? Unlocking this strange union would subsequently unlock the mystery of Crohn’s etiology, still speculated upon 75 years after its baptism.”
I think it is now obvious. It is fish consumption; but particularly fish that is high in vitamin A.
What’s with Manitoba and Minnesota? I don’t know. Maybe they have a higher rate of dairy, or beef liver consumption? They do have a large Native First Nations population in Manitoba. But, conversely, the incidence rates in First Nations people should be statistically lower. This is because most First Nations people are lactose intolerant. That would remove a big dietary source of vitamin A for this group. I don’t know if these are factors in the Manitoba data or not.
Amiens France? Maybe it’s a combination of pâté and coastal fish consumption.
Of course it is not just the fish. It is any source of vitamin A, and I think carotenoids too. The uptick in incidence rates we are seeing in India and China is simple to explain. They are adopting a new western food crop; big time. It is tomatoes. Check the stats; it is amazing, and alarming to see that these countries with huge populations are showing increases in these diseases.
Naturally, it is not just India and China that are eating more tomatoes. It is us here in Canada, and the US too. Business is booming for tomato growers worldwide. Consumption in North America has more than doubled in the last 15 years. What else has doubled in the last 15 years? Crohn’s and Eczema to name a few. The other food business that is booming is the carotenoid based food colors. This is shocking; it is more like exponential growth in production, its use is being mandated and legislated worldwide. Then of course, we have had supplemented milk and dairy since the 1970s. This all adds up to exponential consumption of Vitamin A, and the vitamin A precursors.
This report also points out that the Canadian province of Alberta is quite high in Crohn’s rates too. Why? Well, Alberta is a highly affluent province. It also has quite a high average level of education. So, there is not much of a shortage of money here for the family grocery budget. Therefore, people both listen to nutritional advice, and we have shopping carts that are full of the brightly colored fruits and vegetables; and lots of meat, eggs, dairy, etc., and undoubtedly multivitamins too.
I was at a Costco store here just a week ago, and there was a two pallet (1m x 2m x 1.5m) pile of guess what being sold? Cod Liver oil. There you have it right in the main aisle of the local Costco store. We don’t need an East Coast Fishery to catch the cod. We are supplementing with the worst part of it!
North South Gradient in the Geographic Data
The reports document an observation that there is a World North South gradient in the geographic distribution to the incidence rates of Crohn’s.
There are some really important points to be made about the North-South gradient observation. Firstly, it is not just the rates of Crohn’s disease that present this pattern. The incidence rates of Multiple Sclerosis and type 1 diabetes show up in the same pattern too. Secondly, it is not just a North American phenomenon either. It is present in Europe, Africa, and Australia too. This has nothing to do with genetics. It has to do with the latitude you live at. Is this for real? The more north or south you live at on the earth increases your chances of getting an autoimmune disease. How can this be? Less exposure to sunshine and vitamin D possibly?
No, I think this is going to correspond to the North-South temperature gradient in the Atlantic ocean; and the North Sea. In the case of Chile this is the cold Antarctic ocean. An interesting bit of historical trivia is that Charles Darwin’s condition significantly worsened as he sailed down the coast of Chile, some 200 years ago. We were warned.
The colder waters are going to require fish to have a higher oil content; and I think therefore, a higher level of Vitamin A.
In addition to the North South gradient, I think there is going to be a correlation between incidence rates and the proximity to coastal waters. There sure is in Canada.
I was in Denmark a number of years ago. Eel was popular in lunchtime sandwiches there. At 3,787 IU / 100g; Eel is also very high in Vitamin A. This animal lives in very cold waters. What are the rates for these diseases in Denmark, and the other Scandinavian countries?
Where in the world is the biggest disparity in the incidence rates of Alzheimer’s disease? It is between Finland and just across their border in Western Russia. This border would have been completely closed during the cold war era. The diet in Finland was, and probably still is very high in fish. Their Russian neighbors had next to none; as are their rates of Alzheimer’s disease. Today the Alzheimers/Dementia Death rate (age standardized) Finland / Russian ratio is 34.9 /1.6 per 100,000. But this border region in Russia is even lower than 1.6. Here we have a population with high vitamin A consumption, and they are 22 TIMES higher in their rates of Alzheimers/Dementia compared to their immediate neighbors. Finland also has one of the highest rates of eczema in the world. A really interesting number to find out would be the actual ratio of vitamin A consumption between these two populations. I’m betting it’s going to be close to 22.
Autoimmune diseases are now one of the leading causes of death in North America. These are horrible, and unnatural deaths. If you don’t die from one of these diseases, you are probably going to have a family member that will. Die, or not, Crohn’s, or chronic Eczema, or any other auto immune disease will destroy any young person’s quality of life. We have to stop the insanity.
Is this too simple, and too bizarre to be believable? Well I think not. Once you fully grasp those three simple facts;
your body stores vitamin A
it has a fixed capacity to do so
vitamin A is scientifically documented as a direct toxin and to invoke the immune response that destroys tissue
Then the rest is not too hard to believe; I hope.
Let’s add more evidence.
key evidence: Osteoporosis
Of course Osteoporosis is a common symptom reported with IBD, Lupus, and other autoimmune diseases. Why is that? Well, blocked vitamin D, and therefore calcium absorption is now proven to be a factor in people with elevated levels of Vitamin A. But, I think that is only part of the story. What about all the retinoic acid that is being generated? This will bring down the pH level, and the body’s pH regulation mechanisms need to kick in to counter this. Therefore, I think it is logical for the body to draw calcium from the bone stores to bring the pH level back to normal.
Here is some other great clinical evidence to support this.
Biopsy Interpretation of the Gastrointestinal Tract Mucosa, 2e
“metastatic” calcium deposits that are typical in such patients…. also been associated with hypervitaminosis A …
They go on to state:
“Regardless, mucosal calcinosis itself seems to be of no immediate clinical significance except as an incidental finding in patients with renal failure.”
On the contrary, I think this should be considered to be of huge clinical significance. Where did all this calcium come from? Did it come from the bones, or from the diet? It’s the bones of course.
How long has this been known for? Since the 1940s.
They report high rates of spontaneous bone fractures in rats that are given elevated levels of Vitamin A. It is so toxic that they inadvertently break bones just trying to handle the rats. These rats where fed moderately high levels of vitamin A for only 10 days! The bones were incredibly quickly depleted of calcium.
They noted the consistent occurrence of spontaneous bone fractures associated with hypervitaminosis A and they also noted that no compound other than vitamin A is known to be associated with such fractures in animals.
The highlights are: “The increased risk was greatest among girls and women affected by autism spectrum disorder:
Girls with autism had eight times the hip-fracture rate of other girls.
Women with the disorder had ten times the rate of spinal fracture of other women.
Boys with autism had double the hip-fracture rate of other boys.
Men and women with autism (ages 23 to 50) had nearly 12 times the hip fracture rate of other adults.
Women with autism also had double the rate of arm, wrist and hand fractures.”
Therefore, I think this: “no compound other than vitamin A is known to be associated with such fractures in animals” finding is of huge significance.
Of course, it is not just me that thinks there are a lot of similarities between Autism and Alzheimer’s. I’m going to add another crazy statement into the mix here. Remember that U shaped incidence rate curve I mentioned before; Lot’s of kids less than say 10, and lots of adults 50+ getting eczema. Well we now have lots of kids getting Autism, and a lot of adults getting Alzheimer’s. When combined these two, it presents almost this same incidence pattern.
The current rates of Autism spectrum are now an insane 1/128 kids in North America. Some people claim this is partly due to better diagnosis, and a broader definition of the Autism spectrum. I think that is complete BS!. It is not just a definition that has changed; it is spontaneous bone fractures too!
Since osteoporosis is a universal symptom reported with autoimmune diseases; I think it is important to dig into this topic some more. We really need to understand the mechanism here; or at least come up with a very plausible explanation for it. To do so, firstly let’s revisit the case I cited earlier on in this document of a 6 year old boy being admitted to hospital for hypervitaminosis A. When I selected this as an example case; it was just by pure coincidence that this boy was autistic too. There are some important points about this case we need to consider. Firstly, someone is spreading very bad (criminally negligent IMO ) advice about giving Vitamin A to combat Autism. That is just purely, and simply, absolutely wrong advice; and it could have a devastating, if not fatal outcome.
Secondly, what is really interesting is that the emergency treatment for this boy is to try to get his serum calcium levels into a normal range. This is well documented in the case report. So, why is his serum calcium level so high? We might say, oh well, that is just what is documented to happen with hypervitaminosis A. But why does it happen? I think it is because the excess vitamin A is being converted to retinoic acid. This retinoic acid is causing the huge amount of inflammation this kid experiences; the swollen lips etc. Just as importantly, this abundant retinoic acid causes the serum pH levels be be significantly lowered too. The body must combat this, and combat it fast to bring it back to a normal range. It does this by rapidly drawing in calcium from the bones.
Even though this is a single case study; it completely matches with all the other studies in this regard. What about some really convincing evidence from a broad geographic perspective to support this claim? Well, it turns out we have a recent report from Sweden with just such data. Please watch this video.
Here we have indisputable evidence that elevated levels of Vitamin A are indeed causing osteoporosis. But, the incredibly important point that I’ve been repeating over and over in this document, is the daily consumption is only half of the story. The real risk is the long term elevated storage levels. Also, I want to comment on the statement made in the video that people in Sweden live long and healthy lives. That’s a nice statement, but someone needs to check the stats; since this is not exactly true. Sweden has high rates of autoimmune disease and Alzheimer’s.
Now, with most autoimmune diseases exhibiting this same osteoporosis symptom; hopefully it is not too much of a stretch to make the connection. You don’t have to be in a state of hypervitaminosis A. You just have to have some chronic inflammation. Maybe even just a little extra bit each day. It is going to have a cumulative effect on your calcium stores. Taking more calcium is not the answer; and it could actually be harmful. It is getting the inflammation under control that counts. We need to get to the very basic root cause of the problem.
Weight Gain
Another common symptom reported with Autoimmune diseases is weight gain. Of course, obesity itself is its own epidemic. Therefore, we might easily dismiss that weight gain as just part of living in a developed country. However, for a lot of people with an autoimmune disease; it is beyond this new normal un-normal. Once again; we need to know why. Or least come up with a very plausible explanation. One explanation would be to just say that most people experience fatigue, and therefore don’t exercise enough. Well; in my own personal case; that is not true. I did not experience fatigue for much of the time leading up to my eczema. But, I did have this weight gain creeping up on me. By age 54, I was about 20 lbs overweight. It was going up a few lbs per year, almost regardless of how much exercise I got. It was not too horrible; but still something out of my control was taking over, and causing this happen.
Here’s what I think the mechanism could be. It is a gut bacteria called Bacteroidetes. It is one of the most abundant organisms in the human large intestine. It is observed that when these bacteroidetes populations decline; people become obese. Oddly, and conversely, when people go on a diet, the bacteroidetes populations come back to a normal proportion. The reason this happens is documented to be unknown.
Could it be that there is a common toxin in most of our food that is killing off some of these bacteroidetes? Of course; you know where I am headed with this. If high doses of Vitamin A are a toxin to a human; could very small doses in our regular diet be toxic to this tiny bacteria? Let’s remember that Accutane, and some other acne drugs, are retinoic acid and what it does to bacteria on the surface of the skin. Of course, this is hugely speculative; but I am curious. Since adopting my low vitamin A diet I have lost about 20 lbs. My BMI is now “NORMAL”. I was not fasting at all. I was eating lots, and lots of calories too. The extra weight just magically went away. Go figure?
The Toxicity of Vitamin A – how toxic is it really?
There are tons of scientific and medical publications on the toxicity of vitamin A. Retinoic Acid is documented to be extremely toxic when it is in the wrong place or wrong concentrations. Here is a another really interesting 2012 paper: Retina, Retinol, Retinal and the Natural History of Vitamin A as a Light Sensor stating that “Excessive vitamin A uptake can lead to severe toxicity in humans”.
In the case of Accutane it is extreme. Women taking the drug were required to be on two forms of birth control; or completely abstain from sex. Moreover, they were to enter into a contract; the “I Declare” contract, agreeing that if they did become pregnant; they would immediately seek an abortion. Okay, this is retinoic acid. It is actually a chemo therapy drug! It works by killing rapidly reproducing cells. Did anyone stop to think that normal teenagers have rapidly reproducing cells too? So, what about plain old retinol (regular vitamin A)?
There is a well known study done in the 1990s where pregnant women who were taking 10,000IU or more, resulted in a high rate of birth defects (1 in 57). This was not retinoic acid; it was retinol; plain old vitamin A.
Let’s dig into this a little bit more. What we know for sure is that 10,000 IUs was incredibly toxic. Now, even though 10,000 IUs sounds like a big number, it is actually not. This is only like around 3X the RDA. A person could quite easily achieve this with normal foods alone. But the point is that we don’t know if the 10,000 IUs was the dangerous high level mark or not. It could be 5000 IUs, it could be 3000 IUs. Who really knows for sure? Actually nobody does; because it depends.
Based upon my understanding of what’s happening here is that the real risk is the absorption rates and not the daily dose that matters so much. The absorption rate is going to be very dependent upon prior consumption history, and therefore be a very individual rate.
When you read the various studies on what the safe amount of vitamin A is during pregnancy, they are all considering a daily dose. It is like this is somehow the magic number that needs to be quantified. But, since the body stores the daily dose; I think it is almost the completely wrong number to consider. What is far more important is cumulative storage, and what exactly happens with that daily dose. Additionally; exactly how fast does this process happen. The daily dose number combined with storage level numbers are what are really critical.
Let’s dig into this a little bit more. What we know for sure is that 10,000 IUs was incredibly toxic. Now, even though 10,000 IUs sounds like a big number, it is actually not. This is only like around 3X the RDA. A person could quite easily achieve this with normal foods alone.
But the critical point is that we don’t know if the 10,000 IUs was the dangerous high level mark or not. It could be 5000 IUs, it could be 3000 IUs. Who really knows for sure?
Moreover based upon my understanding of what’s happening here is that the real risk is the absorption rates and not really the daily dose that matters so much. The absorption rate is going to be very dependent upon prior consumption history, and therefore an individual rate.
Generally, older women are probably going to have lower absorption rates; so their risk level is going to be higher. Therefore, the safe amount for pregnant women is also going to be variable just based upon individual dietary habits, and possibly age too.
Let’s imagine what might happen with a well intentioned pregnant woman who wants to do everything she can to make sure her new baby gets all the nutrition it needs. She might eat a few eggs with cheese for breakfast, two glasses of milk, take a multivitamin. She might take an Omega 3 fish oil tablet. Then for lunch a tuna salad. Maybe a salad with lots of brightly colored vegetables such as tomatoes, and bell peppers. Maybe she juices a few carrots with that fancy juicer she has. Boom! Now she surged her vitamin A intake; and maybe way past her safe absorption rate too. Now what? Could some of that excess vitamin A convert to retinoic acid and endanger the fetus? You bet it could!
Fortunately, the medical community is now warning women about consuming too much vitamin A during pregnancy. I don’t know how universally this message is being delivered. There is also the ongoing belief that elevated post delivery Vitamin A consumption is fine, if not being recommended. But, is this really true? Is there 100.00% completely water tight, irrefutable scientific evidence to support this? Or is it just being assumed too? Why on earth do we have this astounding epidemic of Autism in North America?
Okay, in the context of birth defects; someone might claim high doses are only a risk to a developing fetus. But, that is totally incorrect. As you’ve seen here, there is tons of research proving high doses are toxic to kids and adults too. What makes a high dose? Anything that is not nearly immediately stored. Who does this apply to? Kids with small livers, and everyone with current elevated storage. Of course, I can’t just make this claim without strong supporting evidence. So, here it is published in the Journal of the World Public Health Nutrition Association in a May 2010 commentary titled: The great vitamin A fiasco
The findings that high doses of vitamin A, especially in well nourished children, have adverse impacts on respiratory infections, should surely be grounds for serious concern.
I think the critically important point in this statement is the “especially in well nourished children“. Why is this? It is because their absorption rates are going to be slightly lower. This in itself should be hugely telling. There is indeed a very thin range of consumption rates that are safe. This is actually that same higher socioeconomic factor showing up here; but in the context of kids from villages in India etc.
Does anyone think for one second that children in North America are not well nourished too? Does not our supplemented food now load them up with somewhat big doses almost every day?
There is something else about this “adverse impacts on respiratory infections” that needs a bit of investigation. Why exactly does giving a kid a shot of vitamin A cause higher rates of respiratory infections? Isn’t this an amazingly revealing bit of information? It is because surged vitamin A intake leads to inflammation. Inflammation leads to opportunistic infections; especially in sensitive tissues like the lungs.
“In adults, vitamin A deficiency can lead to profound impairment of hippocampal long-term potentiation and long-term depression and impairment in learning and memory. Vitamin A deficiency can also lead to pathological changes in the lung, the skin, the thyroid and the male and female reproductive systems.”
This is very strange, and paradoxical, since this closely matches with some of the major symptoms of vitamin A toxicity. Could, it be that saturated organ storage actually results in a vitamin A deficiency in the brain? Or is the liver no longer able to deliver the vitamin A in the RBP? I have no idea. Whatever the mechanism; vitamin A intake is indeed a double edge sword.
I’ve read another study from 1940 stating that they considered Vitamin A to be so toxic that they recommended that it be a controlled substance. So, this toxicity of vitamin A has been generally well known for a very long time.
Then, for some misguided reason, in the mid 1970s we began adding this well known toxin to nearly all milk and dairy in North America. Then, starting around the 1980s we start seeing this exponential growth rates in disease. We now have an epidemic in Eczema, Crohn’s & IBD, Arthritis, Lupus, Autism, Alzheimer’s, and more. Once again, and amazingly, all the combined symptoms of these diseases are like a perfect match for Vitamin A toxicity. If you have any doubt about this connection; please read on to the Alzheimer’s data I present in the summary.
Does all this make sense, or is it too simple?
Let’s look at the data in the most obvious way. These diseases are doubling at alarming rates. What substance in our food is also doubling at similar alarming rates? It’s easy; just ask the tomato farmers, and the Cod Liver oil suppliers. Then consider that this very bad nutritional advice about eating lots of milk, dairy, and brightly colored fruits and vegetables has taken hold. As so has that horrible advice about supplementing with fish oils. The cited Eczema “trigger foods” are also most of the recommended foods on the Canada food guide.
No, it’s not sugar, or gluten (in itself), to blame here. Sugar will make you fat, but it will not directly dissolve and burn holes in your skin, and organs. Gluten can definitely be an antagonist; but it is not the root cause.
I think there is only one common substance in all of our foods that is scientifically proven to be capable of doing this. It is vitamin A (retinol, and or retinoic acid).
But, you might argue that this is a really simple theory; and there is no way the wider scientific, and medical community is missing this.
Well then please explain to me why alarms were not sent out regarding Accutane? That should have sent shock waves throughout the drug, food, medical communities, and government agencies. But, no, nothing but silence.
So don’t think that some people at drug companies can’t possibly miss the obvious. Not only did they miss the obvious; they completely, and conveniently, ignored over 50 years of scientific knowledge that vitamin A is a toxin at high doses!
Or maybe this vitamin A subclinical toxicity is not obvious? After all, this is a very subtle, and very tricky situation that develops slowly over a long period of time. It is more or less documented to be hugely unlikely to happen on a wide scale like it is. But it is indeed. It is happening, just with unexpected, and with mostly small or, subclinical amounts of this potential toxin being in the wrong place in the human body. Just to be clear here; once again, this is not at all classic Hypervitaminosis A. No; this is a very slow build up to near saturation; and thereafter being in a state of chronic subtle overflow of this toxin.
Or maybe I am completely wrong too? But, everything I’ve presented in this document is not based upon opinion. There are a lot of documented facts; and my own firsthand experiences. I think it should be clear, logical, and compelling evidence.
BTW, I am also now pretty sure what caused the leaking of my kidneys. It is the same horrible yellow toxin that is dissolving, and burning holes in my skin. It is doing the same in the colon, and other internal organs of children, and young adults suffering from Crohn’s, and other autoimmune diseases.
It is time to stop the insanity. Why exactly is kid’s milk, and so many other foods, fortified with a direct toxin? Was this decided by some government bureaucrat decades ago? That may have been fine 40 years ago; but no longer. We have this huge over abundance of vitamin A in other foods. It is time to seriously rethink this. I think we are now seeing the unintended consequences of this; and it is called the auto-immune epidemic.
Why are we selling Cod Liver oil by the truck load to unsuspecting consumers? High doses of Vitamin A have been proven, over and over, to cause birth defects; if nothing else. What the hell is going on?
Is it a coincidence that vitamin A & D have been added to milk and all dairy products since the early 1970s, and the incidence rates for these diseases began skyrocketing in the 1980s? Is it a coincidence that milk and all dairy products are very commonly cited as being foods that “trigger” autoimmune disease flare-ups? Is it a coincidence that elevated levels of vitamin A are now proven to block vitamin D, and that osteoporosis is common in autoimmune diseases? Milk promoting strong bone health is now being proven to be a myth too. Here’s a recent article and a referenced study.
Study Suggests Milk May Actually Increase The Risk Of Bone Fracture
Despite what most people have heard their entire lives, milk may not be so good for bones or for longevity, according to a new study in the journal BMJ. The research found that consuming more milk was linked to greater risk of bone fractures and to earlier mortality. Meanwhile, cheese, yogurt, and other fermented products appeared to be “safe.” It’s not quite clear why, but the research suggests that milk alone may increase inflammation and oxidative stress in the body.
Of course, it is not just the milk and dairy sources. When in human history have we consumed so much of this potential toxin as a regular part of our diet?
Is it a coincidence that reducing a significant source of vitamin A from a million person population results in a 35% drop in the incidence rates of Crohn’s and inflammatory bowel disease?
Is it a coincidence that eczema is a commonly reported co-disease with Alzheimer’s and Autism. Of course spontaneous bone fractures have been documented in vitamin A toxicity since the 1940s. Once again, there is this amazing little bit of trivia : no compound other than vitamin A is known to be associated with such fractures in animals. Why would we think humans are going to be any different in this regard?
Is it a coincidence that the incidence rates of Alzheimer’s have recently dropped a bit in the USA, and Germany too, and both these countries stopped fishing cod off the east coast of Canada.
Is it a coincidence that the United States, Canada, Europe, and other industrialized nations get their vitamin A from multivitamins, fish liver oil, and the fortification of foods such as milk, butter, margarine, breakfast cereals, and some snack foods. Whereas, in the developing nations, 70–90% of vitamin A is obtained from carotenoids in plant based foods. We have an epidemic of autoimmune and other horrible diseases; and they don’t. Does anyone else think there’s a connection here?
The Alzheimer’s Connection
Let’s come back to where we started from in all of this. Alzheimer’s disease rates in Atlantic Canada.
For what it is worth; I actually have very little doubt that this is the root cause of Alzheimer’s too. I know that’s a pretty crazy statement to come from an older engineer / geologist who was just trying to cure a skin rash. And, Yes, I do know that vitamins (including A) have been officially ruled out as the cause of Alzheimer’s disease. So why do I make such an absurd sounding claim?
It is hugely supported in the data; there are very significant correlations with the world geographic and demographic data; very similar to those of Crohn’s and Eczema.
The significant East to West gradient in Canadian rates also means that this is an environmentally induced disease.
Mental dullness, and confusion are well documented symptoms of Vitamin A toxicity. So is memory loss, mental dullness, and confusion with Lupus and a lot of other autoimmune diseases.
People with Alzheimer’s have something like a 40% higher rate of Osteoporosis. Elevated levels of Vitamin A are proven to cause Osteoporosis, and to block Vitamin D; and therefore block calcium absorption.
Vitamin A in the form of retinoic acid is clinically proven to burn holes in tissue.
Once you get into this state of elevated Vitamin A toxicity; it is nearly impossible to randomly stumble upon a diet to get you out of it.
The inflammation on my brain resolved with my vitamin A elimination diet.
My personal cognitive experience with my vitamin A elimination diet.
People with Alzheimer’s commonly report having Eczema too.
I am duplicating that Canadian Alzheimer’s Mortality chart here just for easy reference.
I have no doubt whatsoever that this data is reflecting the closure of the Atlantic Cod fishery in 1993. Also, this data is for mortality rates and I think that the data for age adjusted incidence rates would be even more telling. Clearly the rate changes in NL, PEI, and NB are huge; like almost a 50% decline. Too huge to dismiss as being random, or an anomaly. This represents the entire Atlantic Region of Canada. This is a ~5 million person population with huge decreased rates. This decline is not at all the same in western Canada.
Look at the amazing change in PEI over this time. It has gone from one of the highest rates in Canada to the same rate as BC, and Alberta. I think these Atlantic region numbers would tell a even more amazing story if I had the data going back to 1996, and through to 2014.
Once again here is the chart showing just the Atlantic provinces and with the Nova Scotia Crohn’s Incidence Rates included. Click on the chart to get a better view.
Clearly, something dramatic has changed in Atlantic Canada to cause this steep decline in disease rates. What bigger environmental change has taken place in the Atlantic region in this period of time other than the closure of the Atlantic Cod fishery in 1993? Of course all of that Atlantic cod fish catch was not consumed in the Atlantic Provinces. Some of it was exported across Canada, the USA, Germany and elsewhere. However, enough of it was being consumed in Atlantic Canada to now show up in this data. But, once again, it is not the fish to blame; it is the vitamin A in the fish.
The somewhat anomalous rate change in Nova Scotia as compared to the other Atlantic Provinces might be explainable based on people being diagnosed in the region moving to Halifax to get better access to health services, or long term care facilities. But, that explanation is pure speculation on my part; I have no idea.
Nevertheless, the decline in the Nova Scotia Alzheimer’s rate are pretty significant too. It would be fantastic to see the incidence rates of other big autoimmune diseases in Atlantic Canada being included on these charts. Please help if you can.
Additionally, I think this data from Atlantic Canada makes it perfectly clear that Alzheimer’s is an environmentally (specifically food) caused disease. Therefore, I think that the current research into linking this with genetics, and the various brain banks from victims are almost pointless.
I think that Alzheimer’s is actually going to be a much more subtle and lower level of saturation than what causes Eczema or Crohn’s. It is a subtle chronic little poisoning persisting over decades and decades; with devastating effects.
Is there really a vitamin A to Alzheimer’s causal association here? What we do know is that when we increased vitamin A consumption (via accutane) Crohn’s rates went significantly up. When we decreased vitamin A consumption (via cod) Crohn’s rates went significantly down. We also know that the full set of symptoms of IBD / Crohn’s is a near perfect match with those of vitamin A toxicity. Therefore, based upon the remarkable correlation between the declining trend lines for these two diseases in this one geographic region; in a multimillion person population, a causal relationship is a very strong probability.
Now, having the very important firsthand experience in having the inflammation on my brain vanish after elimination of this substance from my diet; I can move this probability even higher.
I still would not make the call if it were not for a very important, and another amazing connection here. Sadly, this information has been literally staring doctors in the face for many decades now. It is on the faces of people suffering from this disease. It is also on their hands. It is called Eczema. Once again, it is one of those incidental things commonly reported with Alzheimer’s, and Autism too. It is probably considered to be of no immediate clinical significance, not related, and just an annoyance.
If you read the Alzheimer’s caregiver forums, you will see lots of comments about people struggling to treat Eczema. I read one comment about a man caring for his ailing wife, and he could no longer afford all the band aids he was using on her hands. Now, why does a person with a brain disease need band aids on the hands?
I inquired about this Eczema connection with a prominent Alzheimer’s researcher. He simply stated that the observed skin lesions are not related. But, he cannot validly make that claim without first knowing the real root cause of Alzheimer’s. I read another doctor’s rationalization about this observation of the skin problems seen in Alzheimer’s patients. He claimed that it is likely due to these patients not eating properly, and not getting enough nutrition. But, this too is completely not true. Most of these people are well cared for. And there are many incidences in people with early onset; who are still working, and looking after themselves. These people are eating just fine. Nevertheless, to test his hypothesis a bit, I looked at more than a thousand pictures online of anorexic people. Now, these people are indeed starving themselves, and clearly not getting enough nutrition. I could not find a single photo, not one, of an anorexic person showing signs of eczema or psoriasis. Oddly, in nearly all photos the skin looks perfectly clear (other than the skeleton poking through). No eczema, no psoriasis.
Two photos of people had what looked like acne; but they also looked extremely ill. And, no I am not at all recommending people use this as a form of treatment!
A man named John
Here is a video of a 49 year old man from Columbia, with Alzheimer’s. Before playing the video; please look at this first frame very carefully.
There are more close ups of the man’s face and fingernails in the first 60 seconds of the video . Look very closely. What do you see? I see the thickened, and reddish brown skin on the sides of his forehead. I see the mottled fingernails. Does this look familiar? There are a lot of people with eczema who will not only recognize this condition; they will know exactly how it feels too.
Now, I think we can make a pretty good guess as to why the outer 1/3 of the eyebrows go missing in Hashimoto’s disease. Yes, yet another autoimmune disease, this one attacks the thyroid. It has an odd, and incidental skin issue showing up on the face. Weird huh? The immune system is attacking the thyroid, yet burns off the eyebrows too? Does this not seem incredibly strange that the immune system, after millions and millions of years of evolution, would waste its energy and resources like this?
Autism and eczema
There is also a big connection here between eczema and Autism. There are exactly the same type of comments in the Autism support forums. You have all these mothers discussing and sharing tips on how to care for their Autistic kid’s Eczema. Eczema goes hand in hand with Autism. And so does gut inflammation. Why is that?
It is because the root cause of these diseases is indeed hugely related. It is the sub-clinical saturation, and the elevated non-liver storage of retinol and / or retinoic acid. So, based upon that; and my own personal experience, and combined with this data; I am going to say; that there is an incredibly good chance of a causal association here. No, it is not conclusive, but some empirical evidence, that’s almost trivial to obtain, can solidify it.
Of course we should understand the mechanism of how elevated levels of this potential toxin is getting into, or affecting, the brain. My theory is that the process is nearly identical to what is happening with the fats in the sebaceous glands of the skin and GI tract. The excess retinoic acid is a fat soluble molecule. Therefore, it is going to be wrapped in a lipid. The brain is highly dependent upon lipids. Now we have lipids circulating in the blood that are effectively little toxic Trojan Horses. They contain the retinol or retinoic acid molecule. Just like with the skin, the fat is consumed, unwrapping and exposing the toxic molecule. Once exposed, this toxin is going to cause inflammation and destroy tissue, and possibly the build up of proteins.
Also, this same inflammatory process is going to happen anywhere in the body where these toxic lipids are consumed.
Regardless if this is even close to the correct mechanism or not, it does not really matter in the short term. There are lots of times in science we can make use of information we don’t fully understand. For example, I am sure that there are lots of effective drugs in use where their exact mechanism is not fully understood. What is critical at this point is that we actually do something with this information.
There is another personal observation that I want to share. Around 2006 I had almost completely stopped dreaming at nights. I might of had dreams 2 or 3 times in a year. So, that is about 9 years of almost never dreaming at nights. I assumed this was due to drinking too much coffee; or just something that happens with aging.
Four weeks after being on my vitamin A elimination diet; I started to dream every night. That is every single night in about four months now. My coffee intake has remained the same. Of course it was not just dreaming that changed. As stated above, my thinking clarity significantly improved too with my vitamin A elimination diet. Okay, so that is subtle inflammation / pressure on my brain resolved, thinking clarity back to normal, and resumed dreaming at nights.
Do you think this toxin was having an adverse affect on my brain?
With everything I’ve documented here regarding Alzheimer’s; now these two world maps should be very interesting.
I’ve changed the default color coding in Alzheimer’s/Dementia map from red to yellow; just to make the visual correlation easier. Yellow regions in the upper WHO-VAD map are getting lots of vitamin A; and yellow regions in the second map are getting high rates of the Alzheimer’s/Dementia.
Naturally, we all know that correlation does not mean causation. But it does, nevertheless, add supporting evidence to this theory. At the very least, there should be zero doubt in anyone’s mind that Alzheimer’s/Dementia are environmentally induced.
A Thought Experiment
Let’s look at this logically, and go through a bit of a thought experiment together. Please point out where I am making mistakes in logic, or where I am making erroneous, or unreasonable extrapolations.
Okay, let’s start:
Epidemic rates of these diseases in the Industrialized world means they are not genetic.
People immigrating from non-industrialized countries; adopt the same rates of disease here; at least by their second generations. This means it is environmental; that should be perfectly, 100% clear. Therefore, it is probably one or more toxins in food and /or water we all consume.
The exponential rate of increase of Alzheimer’s disease in the USA.
There is something else critically important to be observed from the Alzheimer’s charts shown above. That is the age of onset is moving to the left on the timeline. Alzheimer’s in people less than 50 years of age was almost unheard of just a few generations ago. Now, in Canada, we have something like 50,000 people with early onset. Alarming as that new early onset may sound; that is not what I am pointing out. This shift to the left on the timeline tells more. This is clearly telling us that not only is Alzheimer’s an environmentally induced disease; but one that is related to exposure time! The more exposure, the younger the onset is possible. This means there is really nothing preventing this disease from happening to people in their 40’s, or 30’s etc. The same applies to the autoimmune diseases.
Big regional differences in these disease rates means the toxin is not being uniformly consumed. There is zero chance that this is not environmentally caused.
The dramatic increase in these disease rates started in around the 1970s. Therefore, more of the toxin(s) started to be introduced and/or consumed in the 70s and 80s.
These are not modern day diseases; though the epidemic rates are. Therefore, it is not a modern day toxin(s).
There is clearly a time delay (usually in decades) between consumption, and disease onset. Therefore; it is not a toxin at low doses. The body therefore must be able to deal with a certain amount of this toxin; yet it probably accumulates. Therefore, additionally and oddly, the accumulated amount is not toxic.
The autoimmune diseases affect children and adults; therefore, they are not diseases that result from aging. However, for most adults, once acquired the diseases are chronic (usually remainder of life). Therefore, there is a tipping point or threshold to the level of toxin(s) the body can deal with.
These diseases are very widespread in the industrialized world; there is no geographic region in North America that is immune from these diseases. Therefore this toxin(s) must be very widespread, and very common in the food and/or water we all consume. This is also supported by the fact that very few adults spontaneously fully cure from the disease; meaning that almost no one randomly stops consuming this toxin(s).
The incidence rates are higher in North America along the Atlantic Coast. Therefore, there must be more of this toxin consumed in this region. Other countries, such as the Scandinavian countries, with high rates of saltwater fish consumption have high rates for these diseases too. Therefore, this toxin could likely be found in fish. The two most unanimously cited other trigger foods are milk, and tomatoes. Therefore, this toxin should be found in these two foods too.
Women get these diseases more than men, therefore, they are either consuming more of this toxin, or have a lower threshold for reaching a tipping point.
What is the Immune System telling us?
Nearly everyone in the medical community tells us; and 10’s of millions of people know first hand, that these are triggered autoimmune diseases. Let’s set-aside the apparent oxymoron for now, and note that the most commonly cited triggers are food.
Next; we need to know what functions the immune system provides us. It protects us from viruses, bacteria, fungi, parasites, and toxins. We know with a high degree of certainty that autoimmune diseases are not caused by viruses, bacteria, fungi, or parasites. So, that leaves us with toxins, or the medically accepted view that immune system has somehow become defective. But, the flare-up nature of these diseases clearly indicates that it is not a permanently defective immune system. It is almost randomly defective. Additionally, it is most actively defective when we eat trigger foods, and / or in the winter months. So, it is highly likely that the immune system is actually responding to a toxin; or somehow the defective immune system now knows how to tell the weather.
There are something like 10 million kids with eczema in North America. Although most cases are mild; it is indeed this same autoimmune disease. Is not this in itself very strange? Why do so many kids have an autoimmune disease?
But, magically, most kids “grow out of it”. So, they have a defective immune system for a while, and then it self corrects? Or, more logically, their bodies are able to adapt to, or outpace the consumption of the toxin. But, we know that they are probably not adapting, because for a quite a few of these kids their eczema returns in their 20s, or later in life.
So, I think that the immune system is telling us that we are still looking for a toxin, and most likely one found in food, and weirdly one that is more active, or consumed more, in the winter. Even more strangely, one that only kids routinely grow out of.
The autoimmune diseases such as Crohn’s, Colitis, Lupus, Arthritis, and Eczema all involve the skin either as a secondary or primary symptom. Therefore, this toxin must be documented to affect the skin in the exact same manner.
The combined documented symptoms for these diseases is something like:
Abdominal pain, cramping
Diarrhea
Nausea and vomiting
Diminished appetite and weight loss
Fever
Anemia
Chronic Fatigue
Skin lesions, peeling, nodules
Swollen lips with fissures
Eye inflammation, blurred vision
Joint inflammation and pain
Muscle stiffness
Mouth Ulcers
Bone pain
Osteoporosis; spontaneous bone fractures
Mental Dullness, confusion
Light Sensitivity
Liver issues
Kidney issues
Therefore, the toxin(s) we are looking for should be documented to produce all of these very same symptoms and it must be very widely consumed. That is one hell of a list to match.
Yet, amazingly, there is such a toxin, and it is in nearly all of our foods. It is Vitamin A. It is also essential, and harmless at low doses. It also has a threshold, or tipping point when it becomes toxic. The normal function of the human body is to store and accumulate this substance. It is also high in certain fish. It is also added to all low fat milk, dairy, and margarine, and this policy started in the 1970s. More importantly, the fish oil craze started around the mid 1990s. Consumption of fish oils is exponential in growth in North America.
Why have we done this? Have we now become like Finland in our consumption of fish oils? Is this really good for us? How much of this Omega 3 is from fish or krill oil? Has its vitamin A content been removed prior to packaging? I don’t know.
Health experts commonly tell people that oily fish have more health benefits than white fish. However, their recommendations have never been compellingly proven scientifically in large population studies.
The FDA limits the maximum amount of Vitamin A in multivitamins to 1000 IU??. This is to lower the risk of people accumulating too much of it. Could all this Omega 3 oil be another highly concentrated source of vitamin A that has snuck under the FDA’s vitamin A radar so to speak?
Countries with low vitamin A consumption, or have a vitamin A deficiency, have incredibly low rates of these diseases compared to North America.
If I am right about this; and nothing changes, then we as a society are in very big trouble. The doubling rates we now see for these autoimmune diseases are nothing yet. The doubling rates are not going to be linear.
The body’s absorption rate for retinol is going to follow an exponential decline curve; since it is going to be proportional to remaining storage.
Mathematically speaking; it is therefore going to be exponential, and not linear growth rates in these diseases. The vitamin A consumption rates are zooming too. Therefore, we are headed for a national disaster. It is going to be far more than doubling of rates over the next 10-20 years. It is more likely going to be 4x, and then 8x, etc. every 10, or 20 years.
What are we waiting for? We now have something like 30 or 60 million people with an autoimmune disease in North America. In 20 years, this will cripple our economy; in addition to the horrible pain and suffering. We have to solve this.
As I’ve stated above, this is also not just about Crohn’s and Eczema. I think it is about Alzheimer’s, and quite likely Lupus, Arthritis, Rosacea and probably Psoriasis too. I hope we can add Fatty Liver disease, and some forms of Kidney disease to this list too.
Summary
If the evidence I’ve presented here, and what is in the referenced studies is not enough to convince people that this is at least possible. No problem.
It is almost trivial to prove, or disprove, all of this. We just need a few people with Eczema, and Crohn’s to adopt a zerovitamin A diet for 4 weeks; as a starting point. I believe the same is going to apply to Dementia / Alzheimer’s sufferers too.
The results will be stunningly clear to them. More immediately, people with these diseases just need to reevaluate themselves in the context of the wider list of symptoms documented for vitamin A toxicity. I think they will see the connection.
Of course, I’ve gone past this just being a theory. I think I’ve proven it on myself, with my vitamin A elimination food experiment. But, it’s still early. There is no way to prove a negative; so I cannot guarantee I won’t regress again.
Therefore, I don’t want to give people false hope. I am just one person with one result. Even though the result is very positive, and very compelling; I am not 100% cured either. I am not even going to think about calling myself cured until I am completely symptom free for at least a year; or maybe two years; and my skin no longer glows under my fluoroscope.
This is complicated. It is going to take much, much longer than 4 weeks to fully detox the skin and other organs of this toxin. I have no idea how long it will take; or if it is even truly possible at all to get back into a normal state. The only scientific documentation I can find regarding this elevated adipose tissue condition simply states vaguely: “it is going to take a long time”. However, there are some documented cases of chronic vitamin A toxicity where it had taken something like 7-8 months to fully recover.
Just for the record; I’ve been on a near zero vitamin A diet for nearly four months. I am still alive, and doing quite well. I’ve not used one speck of steroid cream, or any other drug, in that time. Of course, I am now back to consuming plant based foods with small amounts of vitamin A. You can’t be on zero vitamin A consumption for an extended period of time. I think three or four months should be the outer limit.
Therefore, do your own research too. Dig through the reports I’ve cited; and all the other material you can find. See the pictures in my personal account of my food experiment; and recovery from Eczema. Read about the light sensitivity, and fluorescence of retinol and carotenoids. Read about the carotenoids being used in food coloring; and understand that beta carotene is just a double ended retinol molecule. Research the surging growth of tomato production in India and China, and the diet changes in Chile etc. etc, etc. Let the evidence speak for itself.
My only advice is to get the heck off all even slightly high sources of vitamin A; at least until we get to the bottom of this. You might want to stay out of bright sunlight too.
My vitamin A elimination diet
Throughout this document I’ve referred to my vitamin A elimination diet. This was really just started as a very long-shot type of experiment, with the only goal of maybe reducing my eczema condition. Have you ever heard of a person adopting a vitamin A elimination diet? Or a person with an autoimmune disease adopting such a diet? I’ve documented this diet, and my experiment with it, over on my eczema posting. The short version is shown below.
My vitamin A elimination diet:
Water
White or Brown Rice ( not yellow or golden! )
Egg Whites
Beef ( steak, roast, no sauces, or spices other than salt and black pepper if wanted)
Olive Oil ( 2 teaspoons per day )
Black Coffee if wanted ( no milk, no cream, no whiteners )
Vitamin C supplements ( recommended )
Cashews ( 5-10 per day, recommended)
NOTHING COOKED WITH BUTTER or COCONUT OIL. No sauces, no ketchup etc!
This is 3 meals a day, 7 days per week. Eat as much as you need to; but more is not better.
That’s it! Absolutely nothing else! No fish, fish oil, no fruits or vegetables. No cod liver oil, no omega 3/6 etc. from fish sources. No multivitamins, No coconut oil. NOTHING, Absolutely NOTHING else!. Not a single bite, not a speck, not a crumb of anything else. Yes, this is extreme. Admittedly maybe too extreme. However, until we get to the bottom of it; take no chances. If someone knows of a more sensible, and safe means of detoxing off this; I am all ears. Just to be clear, the maximum extent of my medical knowledge is putting on band aids. So, please apply your own good judgment to this.
But, here’s the kicker in all of this. Let’s just say for argument sake that I am completely, and totally wrong about this theory of subclinical toxicity of retinol buildup. Let’s say it is something else that I’ve removed from my diet; like sugar, or gluten. Let’s say that Vitamin A has nothing whatsoever to do with this. Flippantly, I might say who cares what it is?
What I do know with 100% certainty, that by adopting this diet I eliminated chronic fatigue and inflammation on my brain. I eliminated brain fog. Does anyone think that sustained inflammation on the brain is a good thing? We are not talking about resolving a case of foot fungus here.
I eliminated the inflammation on my brain in 3 weeks with a diet change. It is a completely harmless, and simple diet change that anyone should feel comfortable trying for say at least 4 – 8 weeks.
I hope that once we tip over one of these “autoimmune” diseases, the others will fall over like dominoes. Please help push the first one over. This can be done almost completely by the people suffering from these diseases; at least for the critical first stage, of just proving; or refuting this. It is a diet change we are talking about here. No drugs or medications are needed.
Please read my eczema, and other posts on this incredibly important topic. Please add more information, and evidence, pro or con of course, to this. Naturally, I am totally open to discussing this with anyone.
Thanks for reading. I hope this helps someone else.
What’s emerged with the COVID-19 pandemic is a peculiar pattern of vulnerability. It’s being widely reported that older people are the most severely affected by the infection and are the demographic most likely to die from it. Whereas, children and teenagers often appear to sail right through the infection with only minor symptoms, or the just having symptoms equivalent to a cold or minor flu. Yet, at the lower end of the age spectrum, say in one and two-year-old’s, the severity of the diseases increases again.
Children of all ages are susceptible to COVID-19 and while their symptoms are generally less severe than those of adults, a small percentage — particularly preschoolers and infants — can become seriously ill, according to a new study.
So, we have this big U-shape in the age-related severity response to getting the infection. This pattern is similar to the incidence pattern of the autoimmune diseases I discussed in my ETFOH eBook.
Figure 9: Pattern of incidence rates of Eczema in the USA
An equally important observation is that many thousands of people have tested positive for having had COVID-19 and yet have remained completely symptom free. Therefore, it’s very critical to appreciate that just getting COVID-19 is not sufficient on its own to cause disease. Clearly, it’s COVID-19 and something else when combined that leads to the disease. What is that something else? We should all be very curious and striving to find out what it is.
In the context of COVID-19 infections, the general assumption is that older people just have weaker immune systems and are thus less able to fight off the virus. Except, it’s not just age that’s the primary factor. Rather it’s a person’s age combined with their pre-existing conditions, or comorbidities, that somehow makes them more vulnerable to having a severe response. Therefore, we can almost right away dismiss that assumption of a “weak” immune system being to blame because it is not at all just older people who succumb to the infection. Some younger people, even in their 30’s, are dying from the infection too. It’s just much more common to have a severe response in these younger people primarily when they have comorbidities. Therefore, the pre-existing comorbidities are the bigger risk factor. The cited highest risk comorbidities are diabetes, obesity, asthma, other autoimmune diseases, and cardiovascular diseases. If you’ve followed my blog for a while now, you’ll know that these are all diseases that I’ve been attributing to long term vitamin-A toxicity.
Let’s see if we can make some sense out of this. Could it be that there’s some mechanism whereby people with a higher level of vitamin-A storage could be more severely impacted by viral infections, and especially that of COVID-19? Firstly, let’s look at some interesting data regarding the liver storage concentration by age. For that, we’ll look at this 1973 study from Mitchell et al.
Source: G. Vaughn Mitchell, M. Young, C. R. Seward, Vitamin-A and carotene levels of a selected population in metropolitan Washington, D. C, The American Journal of Clinical Nutrition, Volume 26, Issue 9, September 1973, Pages 992–997, https://doi.org/10.1093/ajcn/26.9.992
Quite interestingly, here we have a similar U-shaped curve showing up in the data. Note that the horizontal red line at 286 μg/g is the documented toxic level for liver storage. Remarkably, this means that a large number of young children say from 1 to 5 years old are in the toxic range for liver storage. Then, as they get older their liver’s volume increases (roughly as a cubed function of its cross-sectional size) and they outpace the inbound dietary consumption rate. Then, as people get older their liver concentration slowly saturates to where they move into the toxic storage range once again, and through to the end of life. Let’s remember that this data is from back in 1973, just at the beginning of the foolish North American vitamin-A supplementation programs in dairy, breakfast cereals, etc.. Obviously, the liver saturation numbers will be far worse if sampled today. Just imagine the blue U-shaped curve being shifted up higher on the chart to where more people are over the red toxicity line. So, it’s no wonder why so many people are sick and diseased today. They are, by the very definition of the toxic level of vitamin-A storage, beyond that point. This also corresponds quite well with the fact that about one-third of the American population has NAFLD. That’s all bad enough, but could this somehow also make them more vulnerable to viral infections? Well, this has actually been well documented to be the case for a long time. But, for now, there’s one data point on the above chart that we need to focus in on.
What’s documented in the Mitchell study, and in others, is that very young infants have very low (and often even non-detectable) liver storage levels of vitamin-A.
The Amazing Infant Immune System
So, what do you suppose happens to very young infants exposed to the measles virus? Well, amazingly, often nothing adverse happens. That’s correct, they usually remain symptom and disease-free. Their immune system simply clears the virus. Additionally, most of them have probably acquired true life-long immunity from future infections of the measles virus.
Likewise, just what do you suppose happens to a very young infant exposed to the Dengue virus? Well, once again, often nothing adverse happens. Yes, those infants with their supposedly “weak” immune systems just clear the virus.
Next, just what do you suppose happens to a very young infant who is exposed to, and is subsequently infected by, the truly horrifying syphilis bacteria? Very often, they too remain symptom-free, and their “weak” immune systems clear the bacterial infection!
Even more astonishingly, what do you suppose happens to a very young infant who has a finger or toe severed? Amazingly it often grows back! Yes, these very young infants are amazing at surviving and dealing with very adverse events and pathogen attacks. Infants are starting in life with a great, if not perfect, immune system. Sadly, that all quickly changes once the so-called “medical experts” start administering their “health” intervention programs.
Yet, a great misconception persists in medical science in that very young infants are thought to have poorly developed immune systems. One of the primary reasons they make this assumption is because very young kids simply do not respond to vaccinations. Please consider this meta-analyses of the seroconversion rates by age:
Measles vaccination below 9 months of age: Systematic literature review and meta analyses of effects and safety
In a meta‐analyses of 20 papers, the proportion of infants who seroconverted (%SC) depended on the age at MCV1 vaccination. It increased from 50% (95% CI 29‐71%) at age 4 months to 67% (95% CI 51‐81%) at 5 months, 76% (95% CI 71‐82%) at 6 months, 72% (95% CI 56‐87%) at 7 months and 85% (69‐97%) at 8 months.
For the very youngest of children, there is only about a 50% seroconversion (meaning their immune response created detectable antibodies). The seroconversion rates then increase as they get older. Except, this phenomenon is not because their immune system is maturing. Rather, it’s because their serum levels of vitamin-A are creeping up with age too. We know this because the same effect has been studied in fully grown adults. In adults with abnormally low vitamin-A status, they too have a low seroconversion rate of ~50% when administered vaccines. Then, from other studies, we learn that when adults have their vitamin-A levels pre-boosted up before vaccination, then there is a higher “seroconversion” rate of around the more “normal” ~85% rates. Of course, most vaccinations are really low dose deliberate viral infections.
The known low “seroconversion” rate is why most childhood vaccines are delayed until two months of age. Some researchers claim that the extra vitamin-A has “enhanced” the immune response. But, we know that’s not exactly correct. What’s really happened is that the vitamin-A has enabled the virus to more rapidly replicate, and that then results in the “enhanced” immune response. But, do not for one second think that getting a higher seroconversion rate is a good thing to have happen. It’s the exact opposite. It’s clear evidence that higher background vitamin-A levels are resulting in the increased replication rates of the vaccine’s virus. And, vice versa, the run-away viral infection has increased the toxicity of their background vitamin-A levels too.
This is a super, critically, important point to understand. This is the underlying mechanism as to why kids in India and other countries of Southeast Asia can have such a devastating outcome from a measles infection. With high, or even moderate, vitamin-A serum levels, and a lack of sufficient dietary fats and proteins, the measles infection also increases the toxicity of their endogenous and circulating vitamin-A levels! It is also the underlying reason why some kids die when given their vaccines.
What’s going on here? As usual, it’s multifactorial, and there’s much more to the story. What we do know, and also very contrary to widely-held myths, is that vitamin-A actually subdues the immune system. What’s also been documented for like the last 50 years now is that vitamin-A weakens and otherwise damages cell membranes. It also damages the mitochondrial membranes. It’s trivial to see why too. Both the cholesterol molecule and the side-chains of the vitamin-A molecule are made up of isoprene groups. These isoprene groups are the base compound for natural rubber. So, if you’ve ever wondered why the cholesterol deposits surgeons pull out of arteries looks so much like rubber, it is because it is rubber. Ever wonder why the cholesterol deposits are yellow in color? It’s in good part because it has picked up and encapsulated the vitamin-A, and carotenoid molecules, within it.
Carotenoids are incorporated into very low density lipoproteins (VLDL) and exported from the liver into the blood. VLDL are converted to LDL by lipoprotein lipase on the surface of blood vessels. Plasma membrane-associated receptors of peripheral tissue cells bind apolipoprotein B100 on the surface of LDL, initiating receptor-mediated uptake of LDL and their lipid contents.
Source: Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc http://www.nap.edu/catalog/10026.html Page 94
Now, just as cholesterol with its isoprene groups nestles into the lipid bi-layer of the cellular membranes, so too does vitamin-A. This obviously weakens the integrity of the cell membrane.
Could the weakened cell membrane then make the cell more susceptible to viral infections? You bet it can. This has been documented in the context of HIV infections. Supplementing HIV patients with vitamin-A causes a more rapid replication of the virus, and results in worse outcomes. So, we have multiple pieces of real-world evidence that vitamin-A causes a faster replication rate of viruses. What about some laboratory-based evidence? Well, there is indeed, and even specifically for the coronaviruses.
Retinoic acid modification of cell culture used for reproduction of enteropathogenic viruses.
Abstract The 0.001-0.005% retinoic acid injection into the growth cultural medium of prime and continue cell cultures 12-24h before inoculation considerably raised the cell sensitivity to animal entero- and coronaviruses. The entero- and coronaviruses concentrations in cultural medium increased by 10(1.58) and 10(1.68)TCID 50/1.0 respectively. The optimized parameters of the cell culture processing for the enteropathogenic viruses reproduction improvement are proposed.
And a similar phenomenon is observed in the context of Zika infections. Cells being forced into “differentiation” via retinoic acid increased their infectivity to viruses.
Differentiation enhances Zika virus infection of neuronal brain cells
Here we investigated ZIKV infectivity in neuroblastoma SH-SY5Y cells, both undifferentiated and following differentiation with retinoic acid. We found that multiple ZIKV strains, representing both the prototype African and contemporary Asian epidemic lineages, were able to replicate in SH-SY5Y cells. Differentiation with resultant expression of mature neuron markers increased infectivity in these cells, and the extent of infectivity correlated with degree of differentiation.
So, we now have good evidence of vitamin-A (and specifically retinoic acid) promoting the replication of viruses. Of course, we all know that increased background storage levels of vitamin-A simply means more endogenously produced retinoic acid.
None of this is new information. As with most things related to vitamin-A science, it’s been well known about and reported on for a long time. Here’s a great paper from Anthony Mawson discussing the same comorbidity patterns in the context of the 2009 SARS-CoV infections. Back then it was also the people with the pre-existing conditions of heart disease, asthma, and autoimmune diseases who were at higher risks for severe disease and death.
Role of Fat-Soluble Vitamins A and D in the Pathogenesis of Influenza: A New Perspective
Anthony R. Mawson
Department of Health Policy and Management, School of Health Sciences, College of Public Service, Jackson State University, Received 4 April 2012; Accepted 3 May 2012 Academic Editors: M. C. W. Chan, N. Kawai, and Y. Lai
The Symptoms of Influenza A Infection Are Similar to Those of Hypervitaminosis A
As noted, the clinical spectrum of influenza A infection, including avian influenza H5N1, is not restricted to the lung and can range from mild influenza-like illness to severe pneumonia, acute respiratory distress syndrome (ARDS), acute lung injury (ALI), and multiorgan failure [15]. Fever, rhinitis, myalgia, malaise, headache, cough, dyspnea, sore throat, and fatigue are the main presenting symptoms. Complications include pneumonia, bronchitis, or sinusitis, and rarely encephalitis, transverse myelitis, Reye syndrome, myocarditis, or pericarditis [110].
Mawson does a great job of explaining how and why this can be related to an overload of vitamin-A, and why a low vitamin D/A ratio is a very important factor. Oddly, this paper was not picked up by the major journals, say such as the BMJ, or Lancet. Why was there so little interest in this Mawson paper? Could it be that the medical establishment and the pharmaceutical industry have no genuine interest in understanding what’s really enabling and driving viral infections? Could it be that their primary, if not only interest, is their commercial interests? Of course, it is. These companies have multi-billion dollar vaccine divisions. Therefore, any non-vaccine solution to viral infections would be a serious and direct threat to that ongoing annual business model. Therefore, it is incredibly unlikely that we’ll ever see a non-vaccine based solution developed by the pharmaceutical industry. What if we all came to the understanding that the best way to protect ourselves from viral infections was simply to keep our vitamin-A consumption very low? That could devastate the industry. Therefore, that information cannot be allowed to be developed and confirmed. Therefore, the Mawson paper must be ignored.
The ACE2 Receptors
There’s been a lot of press lately about the important role that the ACE2 receptors play in COVID-19 infections. The virus’s glycoprotein binds to the cell membrane protein angiotensin-converting enzyme 2 (ACE2) and that’s how it gains entry into the human cell.
The novel coronavirus 2019 (2019-nCoV) uses the SARS-coronavirus receptor ACE2 and the cellular protease TMPRSS2 for entry into target cells
Here, we demonstrate that 2019-nCoV-SusestheSARS–coronavirusreceptor, ACE2, for entry and the cellularprotease TMPRSS2 for 2019-nCoV-S priming. A TMPRSS2 inhibitor blocked entry and might constitute a treatment option. Finally, we show that the serum form a convalescent SARS patient neutralized 2019–nCoV-S-driven entry.
Not at all surprisingly, retinoic acid upregulates the same ACE2 receptors.
Upregulation of angiotensin-converting enzyme 2 by all-trans retinoic acid in spontaneously hypertensive rats.
However, in atRA-treated SHR, a significant upregulation of ACE2 expression was observed in heart and kidney. In conclusion, chronic atRA treatment increases gene and protein expressions of ACE2
Naturally, with the ACE2 receptor being the target site of virus entrance into the cell there’s been a ton of frantic research into looking into ways to block or down regulate the ACE2 receptors.
Correspondingly, there’s been a ton of interest and media attention given to a well-established anti-malaria drug named chloroquine. Here’s a study from back in 2005 discussing it.
Chloroquine is a potent inhibitor of SARS coronavirus infection and spread
Results We report, however, that chloroquine has strong antiviral effects on SARS-CoV infection of primate cells. These inhibitory effects are observed when the cells are treated with the drug either before or after exposure to the virus, suggesting both prophylactic and therapeutic advantage. In addition to the well-known functions of chloroquine such as elevations of endosomal pH, the drug appears to interfere with terminal glycosylation of the cellular receptor, angiotensin-converting enzyme 2.
Therefore, we can see that when the ACE2 receptors are upregulated, viral infection and replication rates increase. Conversely, when the ACE2 receptors are downregulated, viral infection and replication rates decrease.
Yet, something really strange happened with the medical establishment and the mainstream media regarding the potential use of chloroquine as a treatment. These people immediately started attacking it and doing everything they can to discredit it. Why would they do that? Could it be that chloroquine is cheap, off-patent, immediately available and most of all a potentially competitive alternative to the planned vaccine they have in the works?
Dr. Anthony Fauci almost jumps to the podium and claims that the evidence for its effectiveness is only anecdotal, and there is not enough evidence to support claims that chloroquine is effective in combatting COVID-19. But, that’s not quite true. There are existing clinical trials, and back in 2005, even its probable functional mechanism was understood too. Additionally, with very few other immediate options, why not quickly get going on finding out? Why so aggressively downplay it and try to dismiss it as an option? Who and what is he trying to protect?
Why are we no better prepared today for a viral pandemic than were we in 1918?
The last great viral pandemic to ravish the human population was the so-called Spanish Flu of 1918. So, now over 100 years later, we still don’t have any really effective treatments for viral infections. How can that be? After sucking trillions of dollars out of the worldwide economies the pharmaceutical industry has almost nothing meaningful and effective against viral infections. Sure, they have the horrible DNA, RNA chain terminator class of drugs that they claim to be “anti-viral” in action. But, not only are these drugs very expensive, they come with catastrophic “side-effects” that often decimate the overall health of the patient. They are not “medicines”, they are simply poisons that break the cell’s ability to build any proteins at all.
Fortunately, ER and intensive care teams are vastly more capable today in preventing people from dying from viral infections than compared to back in 1918.
What really matters most right now is finding remedies for people most severely affected by the virus. Contrary to the advice of many “experts”, taking vitamin-A is not one of them. The very last thing anyone one should be doing at this time is supplementing with so-called vitamin-A.
As I discussed in ETFOH, one common theme that cuts across all the autoimmune diseases, and even breast cancer too, is the comorbidity of eczema. At a more fundamental level, and what many others have reported on, is there’s another cross-cutting syndrome, and it’s that of insulin resistance. So much so, that many people feel that insulin resistance is at the root cause of many of the chronic diseases. The very definition of Type II diabetes is insulin resistance and metabolic disease. But, it goes well beyond that. Insulin resistance is hugely implicated in coronary artery disease, heart disease, and surprisingly even the brain diseases such as Alzheimer’s too. You’ve probably heard Alzheimer’s disease even being referred to as Type III diabetes. So, let’s see if we can make some sense out of all of this, and find some plausible common ground and the connections between them.
When I wrote about my theory of obesity causation back in October, I referenced this 2016 report documenting the adipose genesis effect of retinoic acid: Circulating Retinoic Acid Levels and the Development of Metabolic Syndrome.
Source: Yan Liu, Hongen Chen, Di Mu, Jiahua Fan, Jiayi Song, Yuan Zhong, Di Li, Min Xia; Circulating Retinoic Acid Levels and the Development of Metabolic Syndrome, The Journal of Clinical Endocrinology & Metabolism, Volume 101, Issue 4, 1 April 2016, Pages 1686–1692, https://doi.org/10.1210/jc.2015-4038
I was somewhat expecting people to call me out on my use of that study. One of the weird aspects to it was even though the authors documented the adipose genesis effect of retinoic acid; they also concluded that the elevated levels of retinoic acid were beneficial in reducing metabolic syndrome.
Conclusions:
The serum RA level is inversely associated with the development of MetS independently of adiposity and insulin resistance.
So, even though one aspect of that study supported my sub-theory of obesity causation, it directly contradicted my overarching theory that retinoic acid was the real culprit in causing the modern chronic diseases. Of course, there is an absolute mountain of other studies and research proving the incredible toxicity of retinoic acid. To me, at least, something was not adding up here with their contrary findings. But, it is rather easy to see where they go wrong in their analysis.
Here’s the source of the problem stated in the Materials and Methods section of their report:
Determination of RA concentrations
Serum RA concentrations were measured using a commercially available ELISA kit according to the manufacturer’s instructions (catalog number MBS705877; MyBioSource). This assay has high sensitivity and excellent specificity for the detection of human retinoic acid.
Do you see it? They did not actually measure serum RA concentrations at all; rather they measured a biological proxy marker for it. Of course, there’s no such thing as “human retinoic acid” either. So, what are these ELISA kits? They are kits that test for and measure antibodies.
The enzyme-linked immunosorbent assay (ELISA) is a commonly used analyticalbiochemistryassay, first described by Engvall and Perlmann in 1972.[1] The assay uses a solid-phase enzyme immunoassay (EIA) to detect the presence of aligand (commonly a protein) in a liquid sample using antibodies directed against the protein to be measured. Performing an ELISA involves at least one antibody with specificity for a particular antigen.
For example, you could use an ELISA test to detect and measure the antibody proteins to Measles. ELISAs are not usually used to measure and quantify specific compounds such as retinoic acid. Using gas chromatography and mass spectrometry is the more standard technique for identifying and quantifying the molecular makeup of compounds.
Of course, in the human body, most circulating retinoic acid (and retinol too) is bound up in wrapper RBPs. Therefore, what the authors meant to say was: “This assay has high sensitivity and excellent specificity for the detection of the human RBPs for retinoic acid.” So, yes, if the body is building the needed RBPs fast enough, then it will safely wrap up the otherwise highly toxic retinoic acid molecule. When wrapped up in the RBP, the retinoic acid will pose far less of a hazard and people are better protected from it. With this protective mechanism explained we can now understand their observations and paradoxical conclusion.
But, the use of the ELISA test is not some major error on the part of the report authors either. It’s probably a good surrogate test, and it appears to be a rather standard practice. Here’s another report where they’ve done the same, except it’s for retinol RBPs.
Retinol-Binding Protein 4 and Insulin Resistance in Lean, Obese, and Diabetic Subjects
By: Timothy E. Graham, M.D., Qin Yang, M.D., Ph.D., Matthias Blüher, M.D., Ann Hammarstedt, Ph.D., Theodore P. Ciaraldi, Ph.D., Robert R. Henry, M.D., Christopher J. Wason, B.S., Andreas Oberbach, Ph.D., Per-Anders Jansson, M.D., Ph.D., Ulf Smith, M.D., Ph.D., and Barbara B. Kahn, M.D.
Serum RBP4 was measured by an enzyme-linked immunosorbent assay (ELISA) (ALPCO Diagnostics) in groups 1 and 3 and by quantitative Western blotting with purified human RBP4 standards in group 2. Immunodetection was performed with a polyclonal antibody to human RBP4 (DakoCytomation).
In addition to the ELISA, they are also quantifying their measurements with the Western Blot test. But, like, with the ELISA, the Western Blot is another type of test for measuring antibodies. Next, let’s consider their results:
RESULTS:
Serum RBP4 levels correlated with the magnitude of insulin resistance in subjects with obesity, impaired glucose tolerance, or type 2 diabetes and in nonobese, nondiabetic subjects with a strong family history of type 2 diabetes. Elevated serum RBP4 was associated with components of the metabolic syndrome, including increased body-mass index, waist-to-hip ratio, serum triglyceride levels, and systolic blood pressure and decreased high-density lipoprotein cholesterol levels. Exercise training was associated with a reduction in serum RBP4 levels only in subjects in whom insulin resistance improved. Adipocyte GLUT4 protein and serum RBP4 levels were inversely correlated.
This is an important finding as it is tying together serum RBP4 levels, insulin resistance, diabetes, metabolic syndrome, and more. Except, just for now, ask yourself why are they using antibody tests to measure RBP levels? Doesn’t something about that strike you as being a bit peculiar?
To be clear, these are not procedural anomalies. It appears to be a preferred measurement technique. Here’s another study where they use Western blotting to measure serum retinoic acid levels:
Valproic acid combined with 13-cis retinoic acid and 1,25-dihydroxyvitamin D3 in the treatment of patients with myelodysplastic syndromes
Timo Siitonen, Timo Timonen, Eeva Juvonen, Venla Terävä, Anu Kutila, Tuomo Honkanen, Maija Mikkola, Heikki Hallman, Marjut Kauppila, Pirkko Nyländen, Eira Poikonen, Auvo Rauhala, Marjatta Sinisalo, Merja Suominen, Eeva-Riitta Savolainen, Pirjo Koistinen
Of course, using mass spectrometry to measure RA acids levels is more problematic because the retinoid is entirely encapsulated within the RBP wrapper. Therefore, samples first needs to be dissolved in solvents to breakdown the protein shell and washout the embedded retinoids. From there, mass spectrometry can be employed. So, although the ELISA and Western Blot are measuring a biological proxy marker, they are probably more expedient tests and good enough for the purpose of their studies.
Okay, now we need to really think about this. If these laboratory tests used to measure serum levels of retinoic acid, and even that of retinol, are in actuality antibody tests, isn’t it pretty logical that the RBPs are indeed antibodies?
Except, for the last 50 years now, medical science has claimed that the RBPs are specialized transport proteins. The grand theory is that the liver first scrubs retinol out of serum and then sequesters it away into storage for later delivery. On an on-needed basis, the liver then releases the retinol wrapped up in the RBPs for transport. That’s a nice-sounding theory. But, there’s a huge flaw now showing up in the story. That flaw is because a large percentage of the RBPs are actually being built and released by the adipose tissues, and not just the liver. That’s correct, the origin of much of the RBPs is from the adipocytes.
Conclusions
RBP4 is an adipocyte-secreted molecule that is elevated in the serum before the development of frank diabetes and appears to identify insulin resistance and associated cardiovascular risk factors in subjects with varied clinical presentations. These findings provide a rationale for antidiabetic therapies aimed at lowering serum RBP4 levels.
Okay, it looks like the grand theory of the RBPs being transport proteins is starting to fall apart.
“Until 2005, the sole known function for RBP4 was to mobilize retinol from tissue stores and deliver it to vitamin A-responsive cells where it can be converted to retinoic acid for use in regulating vitamin A dependent transcription and functions. In 2005, Kahn and colleagues reported that circulating RBP4 levels affect glucose clearance, with high RBP4 levels inducing insulin resistance (Yang et al., 2005; Graham et al., 2006). Specifically, Kahn and colleagues proposed that adipocyte-derived RBP4 is a signal that contributes to the pathogenesis of type 2 diabetes, linking obesity with type 2 diabetes, as well as other obesity-related metabolic diseases.”
Very importantly, this then brings into question the entire premise of retinol’s “storage” in the liver. That’s because the thought to be delivery protein for it is being generated by, and secreted from the adipose tissues and not at all exclusively from the liver’s “storage” site!
Next, let’s think a bit about the cell’s response to viral infections. When a cell gets infected with a virus, it can very mistakenly start replicating and cloning more of the same virus. But, very often, it also wraps the newly made viruses up in a protein capsid. Some cells can then eject the entire capsid out of itself. Secondly, in response to viral infections the adaptive immune system will usually start to build antibodies to the virus. The goal and function of the antibody is to attach itself to specific binding sites of the viral protein. In doing so it effectively bulks up any free circulating viruses so that they become too large to pass through the cell membrane. If successful, the viral infection is brought under control. Except, now when a cell is contaminated by a toxin, it is by a non-protein based molecule. There are no protein binding sites (at all) to attach an antibody to it. Therefore, as with some viruses, the cell needs to wrap toxic molecules in a specialized hollow-core antibody (or capsid if you prefer). Unlike the currently recognized Y shaped antibodies, the RBPs are more barrel-shaped, That barrel-shape is needed to engulf the entire antigen. Shown below is a model of the RBP with its embedded retinol ligand.
Note the retinol molecule (ball and stick model) nestled inside of the far more complex wrapper (ribbon model) of the RBP. Remember that retinol is too toxic to be in serum alone. Here’s the spacefill model of the RBP showing that no part of the retinol molecule is exposed outside of the RBP itself.
Image created with the PDB ID and associated publication, NGL Viewer (AS Rose et al. (2018) NGL viewer: web-based molecular graphics for large complexes. Bioinformatics doi:10.1093/bioinformatics/bty419), and RCSB PDB.
Therefore, this molecular structure is an astonishing feat of chemical separation and isolation. Not only has the cell’s protein weaving machinery been able to detect and identify a single molecule, but it has also separated it out and wrapped it in a complex protein envelope. Remember too that nature is no fool, and it is not wasteful. This extreme measure of molecular assembly and folding dexterity has to be going on for a very good reason.
Why would the body resort to using such an elaborate and costly transport protein structure? Secondly, if this is truly a transport protein, then how does the receiving cell extract out the retinoid payload when no part of it is exposed to the outside world? And, how exactly does it do it in a toxic-safe manner? Why does the RBP only transport just one molecule at a time? And, once again, why are the adipose tissues generating and secreting the RBPs in the first place? Of course, no one knows the answers to these questions. At best, there are just some unsupported speculations tossed around about it.
“RBP is also bound to a carrier protein, transthyretin. The process by which RBP releases retinol for cellular availability is still unknown and not concisely determined.”
Additionally, if the RBPs are “transport” proteins, that are supposed to be so highly-regulated, then why do they accumulate with age?
The real clincher question is: if the liver is building RBPs to deliver retinol to the other tissues, then why are those receiving tissues then themselves wrapping up retinol in their own internally built RBPs and ejecting it? The current theory of the RBPs being “transport and delivery” proteins makes no logical sense.
Isn’t it just so much more logical that the RBPs are hollow-core antibodies? Isn’t it just more logical that as the body gets exposed to more of a toxic load outside of liver storage, the body builds more antibodies to combat and protect us from that now adipose accumulating toxin? Here’s another study indirectly indicating that’s the case:
Summary
Cellular retinol-, retinaldehyde- and retinoic acid-binding proteins were localized in rat retina during pre- and postnatal development by indirect immunofluorescence.
Source: Immunolocalization of cellular retinol-, retinaldehyde- and retinoic acid-binding proteins in rat retina during pre- and postnatal development De Leeuw, A.M., Gaur, V.P., Saari, J.C. et al. J Neurocytol (1990) 19: 253. https://doi.org/10.1007/BF01217303
What is immunofluorescence?
Immunofluorescence is a technique used for light microscopy with a fluorescence microscope and is used primarily on microbiological samples. This technique uses the specificity of antibodies to their antigen to target fluorescent dyes to specific biomolecule targets within a cell, and therefore allows visualization of the distribution of the target molecule through the sample.
Clearly, the RBPs are very antibody-like. But, since we now know they are not “transport” proteins, is it not highly likely they are indeed antibodies? They have just not yet been recognized as such. The next logical question is: if the RBPs are, in actuality, antibodies, then what does that tell us about retinol? It tells us that it is a toxin!
The famous amyloid plaques of Alzheimer’s disease
One of the key neuropathological hallmarks of Alzheimer’s disease is the accumulation of β-amyloid plaques in the brain. No one knows why they develop or what to do about them. What’s assumed is that they are just defective ribbon structured proteins that exhibit some weird and unexplained misfolding. But, doesn’t that sound a lot like the folded ribbon proteins of the RBPs? Here’s a description of the RBPs
Lipocalins
Members of the lipocalin family, including the retinoid-binding proteins RBP, epididymal retinoic acid-binding protein and β lactoglobulin, share a very low sequence identity but display a highly conserved overall fold. They are composed of an eight stranded antiparallel β-sheet that is folded over itself to form a hydrogen-bonded β-barrel, which constitutes the ligand binding pocket (Figure 2). The N-termini of these proteins are folded around the back of the barrel, `capping’ that side of the pocket.
Next, we need to know and deeply appreciate that it’s not just the liver and adipose tissues that are excreting the RBPs. It’s also happening in the kidneys, lungs, heart, skeletal muscle, spleen, eyes, and testes too.
Functions of RBP
Retinol is secreted from its storage pools and circulates in blood bound to RBP. The main storage site for vitamin A and, correspondingly, the main site of synthesis of RBP, is the liver, although other tissues (including adipose tissue, kidney, lung, heart, skeletal muscle, spleen, eye and testis) express this protein.
Source: Retinoid-binding proteins : mediators of retinoid action Biochem. J. (2000) 348, 481±495 (Printed in Great Britain) 481 REVIEW ARTICLE Noa NOY1 Division of Nutritional Sciences, Cornell University, Ithaca, NY 14853, U.S.A
And then there’s this statement:
The mechanism by which retinol initiates secretion of RBP from cells is unknown, but appears to be conserved in yeast ectopically expressing RBP.
Source: As above
I think it is quite obvious that the cells of multiple tissue types are synthesizing their own RBPs as a protective measure in an attempt to rid themselves of a highly toxic molecule. Do you see where I’m going here? Yes, if the cells of the liver, adipose tissues, kidney, lung, heart, skeletal muscle, spleen, eye, and testis are all able to secrete RBPs, with the retinoid wrapped up inside of it, why shouldn’t we think that the nerve cells of the brain are not going to do the same? Just like the fact that the RBPs are unrecognized as antibodies, couldn’t the famous amyloid plaques of Alzheimer’s disease be unrecognized as RBPs generated by the brain too? Or maybe, since Alzheimer’s is such a new phenomenon in human existence, the amyloid plaques are an ongoing attempted synthesis of RBPs? Thinking that the cells of the nervous system can generate amyloids is not just speculation. As mentioned above, the RBPs are often bound in serum to transthyretin.
Transthyretin
Transthyretin (formerly known as prealbumin) is a plasma protein involved in the transport of thyroxine and retinol and is secreted in great amounts by the choroid plexus epithelium.
Knowing that transthyretin is typically bound up with the RBPs it’s no surprise that so many people with diabetes, autoimmune diseases, and even dementia have the comorbidity of abnormal thyroid functions.
There are some rather remarkable similarities between the so-called defectively folded proteins of the amyloid plaques and that of the folded over proteins of RBPs. For example, here’s the CRYSTAL STRUCTURE OF THE PROTEASE INHIBITOR DOMAIN OF ALZHEIMER’S AMYLOID BETA-PROTEIN PRECURSOR
Image created with the PDB ID and associated publication, NGL Viewer (AS Rose et al. (2018) NGL viewer: web-based molecular graphics for large complexes. Bioinformatics doi:10.1093/bioinformatics/bty419), and RCSB PDB.
As with the RBPs, the Alzheimer’s disease defining proteins adopt a β‐sheet structure and sometimes form into amyloid plaques. Most importantly, when you consider that there has been an 800 times increase in the rate of Alzheimer’s disease since the early 1970s, it is completely, absolutely, undeniably, positively crystal clear that the disease is a poisoning. It’s then easy to appreciate that the cells of the brain are responding to that poisoning in very similar ways as do say the cells of the kidney, lungs, etc. However, once trapped inside the brain, there is no viable disposal pathway for these unusual proteins. The brain just slowly accumulates and clogs up with the amyloid plaques. Not only that, but all the energy and resources wasted in building the amyloid plaques has been taken away from the brain’s normal tissue maintenance and repair processes.
Very tragically, billions of taxpayer-funded dollars have now been spent by researchers going on a wild goose chase of blaming genetics for this disease. Of course, it is a colossal waste of money and time because it is completely obvious Alzheimer’s disease is not caused by genetics. Not only does it take thousands of years for a genetic shift to occur in the human population, the country with the highest genetic diversity on the planet now has the highest rate of Alzheimer’s disease in the world. And who cares about some supposed “genetic predisposition” to the disease because there’s absolutely nothing people are going to be able to do regarding their genetic makeup. So, investigating genetics is pretty much a meaningless distraction from the real culprit of the disease being environmentally caused. If people were not being slowly poisoned by some environmental factors, then their “genetic predisposition” would never be a problem.
Of course, it’s not just the brain that’s clogging up with amyloid plaques, it’s the heart and other organs too. Not at all surprisingly, that also directly correlates to the serum levels of the RBPs!
Identification of Transthyretin Cardiac Amyloidosis Using Serum Retinol-Binding Protein 4 and a Clinical Prediction Model
Findings In this case-control study that included 34 patients with transthyretin cardiac amyloidosis and 77 control participants, retinal-binding protein 4 was significantly associated with the disease independently of tested confounders. A prediction model composed of retinal-binding protein 4, transthyretin, and echocardiographic and electrocardiographic characteristics had excellent discrimination for transthyretin cardiac amyloidosis (deposition of amyloid).
Conversely, the vascularization of the brain in AD patients often shows the same type of damage as that presented in coronary artery and heart disease. The condition is called “vascular dementia.” Therefore, it’s very probable that the same root cause force behind that vascular damage is driving both diseases. Equally important is to know that almost no one dies directly from Alzheimer’s, rather they die with Alzheimer’s. Meaning, the real cause of death is one of their other conditions, such as kidney disease, heart disease, stroke, choking, pneumonia, etc.
Additionally, It’s well documented that persons with Type II diabetes are at a bigger risk (~200%) for developing Alzheimer’s disease. It is even claimed that the single biggest risk factor for developing Alzheimer’s disease is having Type II diabetes. Therefore, many people have made the erroneous assumption that the diabetes is somehow causing Alzheimer’s disease. But, that’s not quite true. Diabetes is not “causing” the Alzheimer’s. Rather, both diseases are simply joined at the hip, metaphorically speaking. And in both diseases we have the common themes of insulin resistance and the development of amyloid plaques. Obviously, diabetes is not “causing” the Alzheimer’s and Alzheimer’s is not “causing” the diabetes. Once again, something else is at the root cause of both diseases. As we’ve seen, elevated serum levels of the RBPs are a significant marker in both diseases too. It is also true for the development of amyloid plaques of the heart. So much so, that it is pretty much an undeniable fact that the RBPs are somehow involved. But, there is an even more direct connection between these two major diseases. As with heart disease, it’s the accumulation of misfolded proteins.
Protein misfolding and aggregation in Alzheimer’s disease and type 2 diabetes mellitus.
AD is characterized by the accumulation of amyloid-β (Aβ) in the brain, while T2DM is characterized by the deposition of islet amyloid polypeptide (IAPP, also known as amylin) within beta-cells of the pancreas.
It is becoming increasingly believed that islet amyloidosis is the progeny of many diseases, including T2DM. The production of islet amyloid polypeptide (IAPP) oligomers that results in amyloid deposition is considered as a major contributor in pathogenesis and progression of T2DM [16]. This has been found present in 96% of T2DM patients and is recognised as a hallmark for diagnosis of this disease.
And then:
LINKAGE BETWEEN AD AND T2DM
AD and T2DM are both prevalent in the aged population. Whereas the cerebral accumulation of Aβ is a major pathological hallmark of AD [168], the deposition of a very different polypeptide, amylin, that likewise succumbs to β-sheet formation and self-aggregation occurs within the pancreas, especially in β-cells, in T2DM.
So now, just what do you suppose is responsible for causing the messed-up structure of the proteins generated by the pancreatic and other tissue stem cells? How about we seriously consider it to be a toxic molecule that has now been proven to cause about 500 different gene “expressions” in stem cells. Except, to most of us here it’s now clear these are, in actuality, sites of gene “damage” and not that of gene “expressions” at all. That gene damage then messes up the cell’s protein weaving machinery. Naturally, the follow-on consequence is going to be the defective structures of the manufactured proteins.
Somewhat like with the wild goose chase of genetics, there’s been a vast amount of research in trying to correct the misfolding proteins using pharmaceutical drugs. Of course, that effort has been futile. Additionally, most research is narrowly focused right down into trying to decipher what’s wrong with the protein structure, Oddy, it appears most people are only asking why the protein is misfolding, as if something has gone wrong with it post manufacturing. They they are not considering that it has been expressly manufactured that way due to RNA/DNA damage.
The RBPs tied-together with Insulin Resistance
GLUT4 – is the glucose transport protein used by cells to take-up insulin from serum. Obviously then if the GLUT4 proteins are not of sufficient quantity or quality, it then will cause the condition of Insulin Resistance. It’s not hard to imagine that if the cell’s energy and resources are tied up generating RBPs, that could be impairing their production and or functioning of the GLUT4 proteins. This scenario is indeed being demonstrated in clinical research. For example:.
Serum retinol binding protein 4 contributes to insulin resistance in obesity and type 2 diabetes.
This now brings us full circle to where I hope it shows how it’s all interconnected. The information presented here not only links the RBPs to Type II diabetes and the amyloid-β plaques; it seriously implicates it in causing coronary artery, heart disease, and of course Alzheimer’s too. Except, we need to be very careful here and not try to blame the RBPs. Rather it’s the overload of retinol that is the very root cause. It’s the overload of retinol that has forced production of the RBPs in the first place. There’s one more connection with insulin resistance that I’d like to discuss, and that is Mitochondrial Dysfunction. There are hundreds of research papers documenting that Mitochondrial Dysfunction and Diabetes are very closely coupled. But, as always, there’s more to the story, and that is the key role of the retinoids directly damaging the mitochondria.
Vitamin A and Retinoids as Mitochondrial Toxicants
Overall, such findings indicate a potential ability of vitamin A and its derivatives to negatively interact with biological membranes, an event that may lead to organelle stress, as, for instance, mitochondrial dysfunction, and to cell apoptosis or necrosis.
‘Vitamin A and its derivatives, the retinoids, disrupt mitochondrial function by a mechanism that is not completely understood. However, it accounts with impaired electron flux between the complexes of the METC, increased ROS production, and induction of oxidative and nitrosative stress to mitochondrial membranes. Additionally, vitamin A and retinoids alter the mitochondrial structure by causing swelling of the organelle. More investigations are needed to elucidate how vitamin A and retinoids affect mitochondria and whether there is a causative link between such event and the clinical manifestations observed both experimentally and in humans.’
Source: as above
Predictably, the thinking from some pharma funded researchers is the same. It’s viewed as an opportunity to try to develop a new drug that will block or intervene in the synthesis of the RBPs. Of course, it always comes down to needing a “drug” to “block” something. Using a non-drug based therapy is completely unthinkable to these folks. But, since we know with 100% certainty that Alzheimer’s is the result of a long term poisoning, the only “drug” that could even possibly work is one that acts as an antidote to whatever that poisoning is. Until then, almost all other drugs are just going to be useless, and most will cause even more harm. Now with the known connections between the elevated RBPs and the development of amyloid plaques, and having a better understanding of RBPs likely being an antibody response to a toxin, isn’t it very likely retinol is the responsible toxin?
Maybe it’s just me, but how about we just consume a lot less of the retinoids and let the body heal itself?
Are the RBPs antibodies? Please have a think about it and comment as you see fit.



































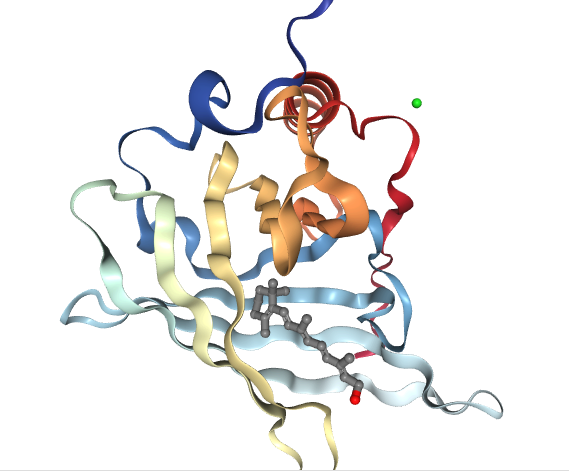
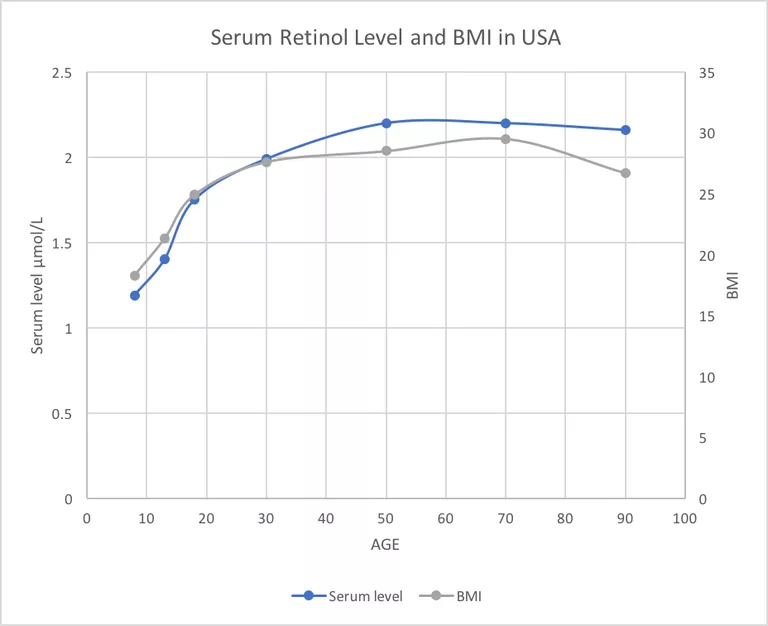
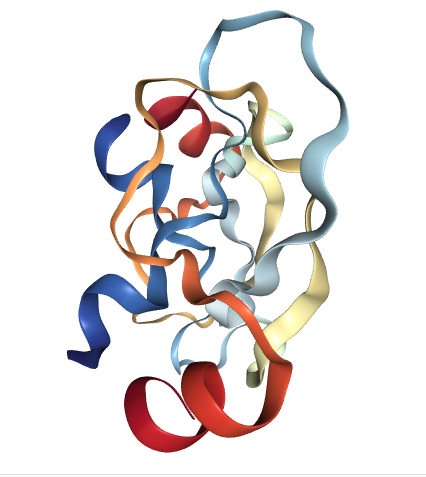
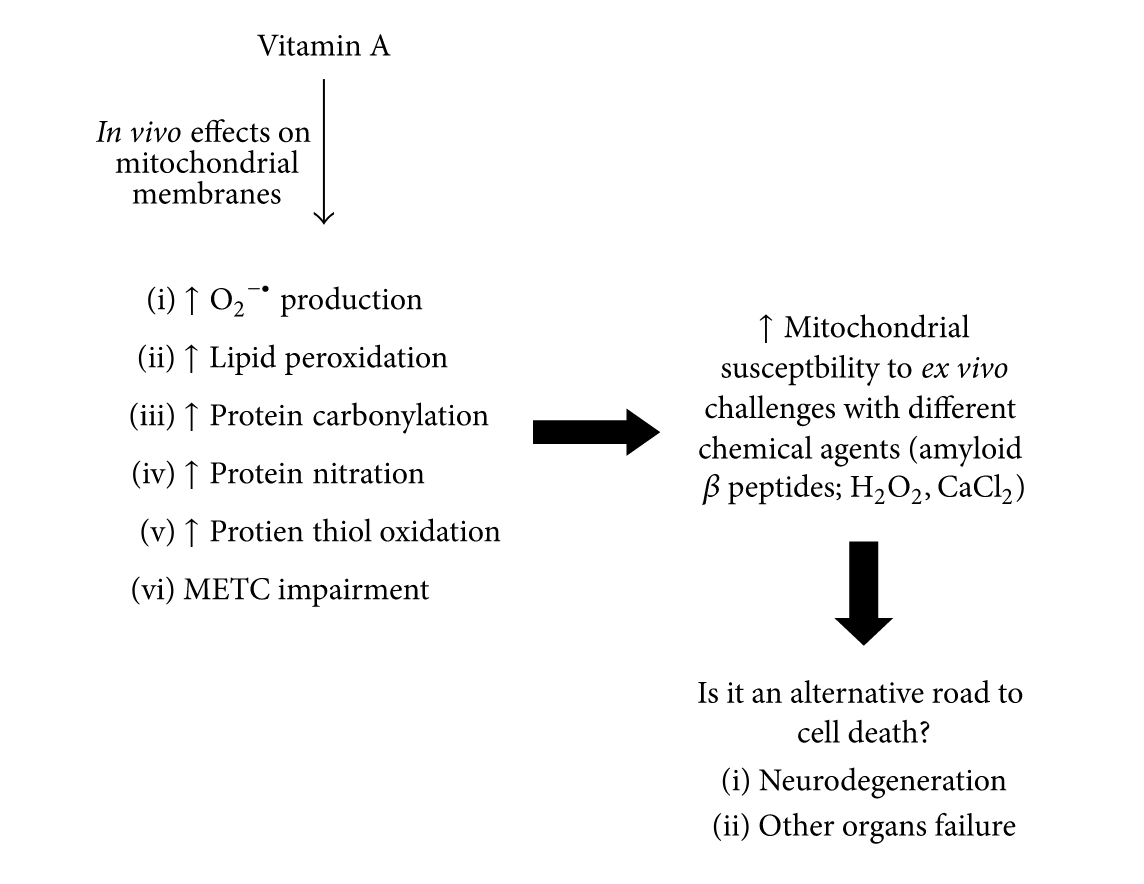

{kind=link}
You must be logged in to post a comment.